

This is a preprint.
Pediatric cerebrospinal fluid immune profiling distinguishes pediatric-onset multiple sclerosis from other pediatric-onset acute neurological disorders
- PMID: 40060552
- PMCID: PMC11888486
- DOI: 10.1101/2025.02.27.637541
Pediatric cerebrospinal fluid immune profiling distinguishes pediatric-onset multiple sclerosis from other pediatric-onset acute neurological disorders
Abstract
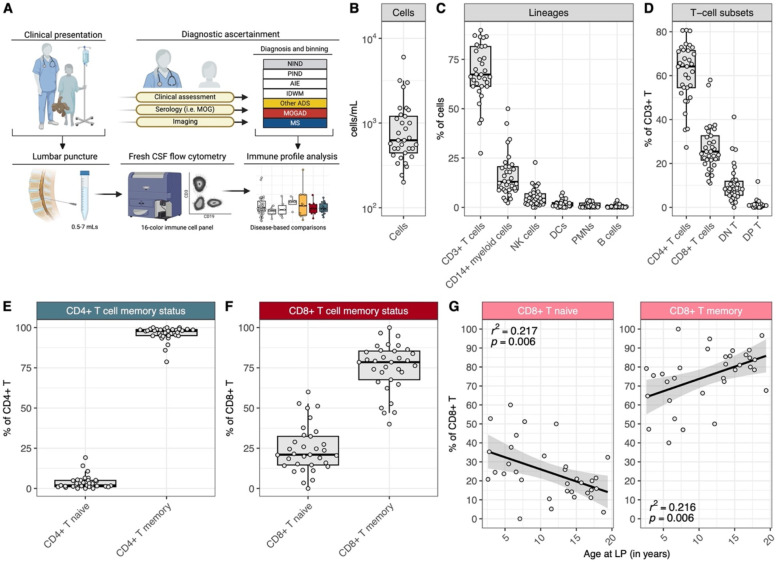
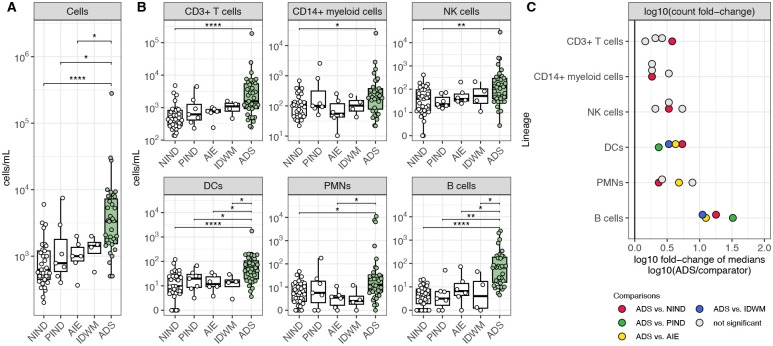
The cerebrospinal fluid (CSF) provides a unique glimpse into the central nervous system (CNS) compartment and offers insights into immune processes associated with both healthy immune surveillance as well as inflammatory disorders of the CNS. The latter include demyelinating disorders, such as multiple sclerosis (MS) and myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD), that warrant different therapeutic approaches yet are not always straightforward to distinguish on clinical and imaging grounds alone. Here, we establish a comprehensive phenotypic landscape of the pediatric CSF immune compartment across a range of non-inflammatory and inflammatory neurological disorders, with a focus on better elucidating CNS-associated immune mechanisms potentially involved in, and discriminating between, pediatric-onset MS (MS) and other pediatric-onset suspected neuroimmune disorders, including MOGAD. We find that CSF from pediatric patients with non-inflammatory neurological disorders is primarily composed of non-activated CD4+ T cells, with few if any B cells present. CSF from pediatric patients with acquired inflammatory demyelinating disorders is characterized by increased numbers of B cells compared to CSF of both patients with other inflammatory or non-inflammatory conditions. Certain features, including particular increased frequencies of antibody-secreting cells (ASCs) and decreased frequencies of CD14+ myeloid cells, distinguish MS from MOGAD and other acquired inflammatory demyelinating disorders.
Conflict of interest statement
COMPETING INTERESTS The authors declare no conflict of interest related to this study.
Figures


References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials