

Commercial hybrid graft versus traditional arch replacement with frozen elephant trunk: A multi-institutional comparison
- PMID: 40061564
- PMCID: PMC11883694
- DOI: 10.1016/j.xjon.2024.10.027
Commercial hybrid graft versus traditional arch replacement with frozen elephant trunk: A multi-institutional comparison
Abstract
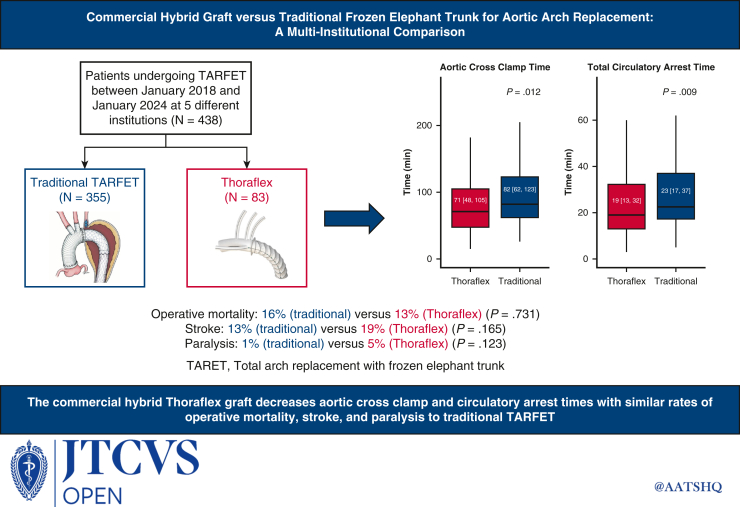
Objective: Traditional total arch replacement with frozen elephant trunk requires 2 separate grafts in the descending thoracic aorta and arch, and frequently requires a graft-to-graft anastomosis, which is prone to bleeding. The Thoraflex (Terumo Aortic) device treats the arch and descending thoracic aorta in a single device but has not been compared directly to traditional total arch replacement with frozen elephant trunk and has not been studied in a real-world context in the United States.
Methods: A consecutive sample of total arch replacement with frozen elephant trunk patients across 5 different institutions between January 2018 and January 2024, identified 438 patients of which 83 out of 438 (18.9%) had a Thoraflex device. Propensity score matching in a 1:2 ratio identified 166 well-matched controls. Groups were compared across perioperative outcomes.
Results: One hundred forty out of 438 (32%) patients presented with acute type A dissection, 112 out of 438 (26%) had an aneurysm, and 87 out of 438 (20%) had chronic dissection with a previous proximal repair. One hundred thirty-two out of 438 (30%) underwent surgery on an emergency or emergency/salvage basis. Median (interquartile range [IQR]) crossclamp times in the Thoraflex and traditional matched groups were 71 (IQR, 48-105) and 82 (IQR, 62-123), respectively, (P = .012). Total circulatory arrest times were 19 minutes (IQR, 13-32 minutes) and 23 minutes (IQR, 17-37 minutes), respectively (P = .009). Total procedure times were 6.1 hours (IQR, 5.2-7.3 hours) and 6.8 hours (IQR, 5.7-8.2 hours), respectively (P = .012). The operative mortality, stroke, and paralysis rates were 11 out of 83 (13%), 16 out of 83 (19%), and 4 out of 83 (5%), respectively, in the Thoraflex group and were not significantly different than matched controls.
Conclusions: The Thoraflex hybrid device facilitates shorter crossclamp and circulatory arrest times for arch replacement, with similar observed mortality and stroke rates compared with matched controls.
Keywords: aorta; aortic arch; frozen elephant trunk.
© 2025 The Authors.
Conflict of interest statement
Dr Fleischman is a consultant for Terumo, Atrivion, Edwards, Cook, and Gore. Dr Glotzbach is a consultant for Terumo, Gore, and Corcym. Dr Reece is a consultant for Terumo, Gore, Atrivion, and Corcym. All other authors reported no conflict of interest. The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
Figures






References
-
- Dake M.D., Miller D.C., Mitchell R.S., Semba C.P., Moore K.A., Sakai T. The "first generation" of endovascular stent-grafts for patients with aneurysms of the descending thoracic aorta. J Thorac Cardiovasc Surg. 1998;116(5):689–703. doi: 10.1016/S0022-5223(98)00455-3. discussion 703-704. - DOI - PubMed
LinkOut - more resources
Full Text Sources
