

Risk Factors, Clinical Course, and Management of Delayed Perforation After Colorectal Endoscopic Submucosal Dissection: A Large-Scale Multicenter Study
- PMID: 40064741
- PMCID: PMC12296770
- DOI: 10.1007/s10620-025-08949-5
Risk Factors, Clinical Course, and Management of Delayed Perforation After Colorectal Endoscopic Submucosal Dissection: A Large-Scale Multicenter Study
Abstract
Introduction: Delayed perforation (DP) remains a significant complication of colorectal endoscopic submucosal dissection (ESD). This study analyzed the risk factors, clinical course, and management for DP following colorectal ESD.
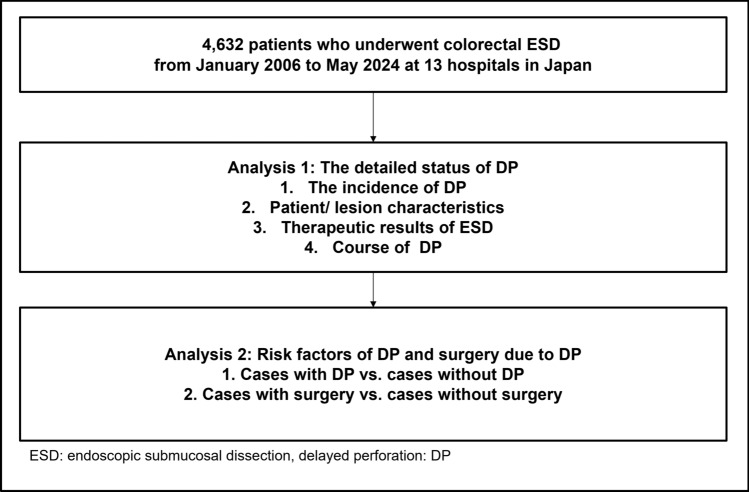
Methods: We retrospectively reviewed 4,632 consecutive colorectal ESD cases from 13 institutions between January 2006 and May 2024. DP cases were identified, and the incidence rate, along with patient/lesion characteristics (as tumor size, location, and severe fibrosis) were assessed. The clinical course, including onset timing, initial treatments, need for surgery, and risk factors were examined.
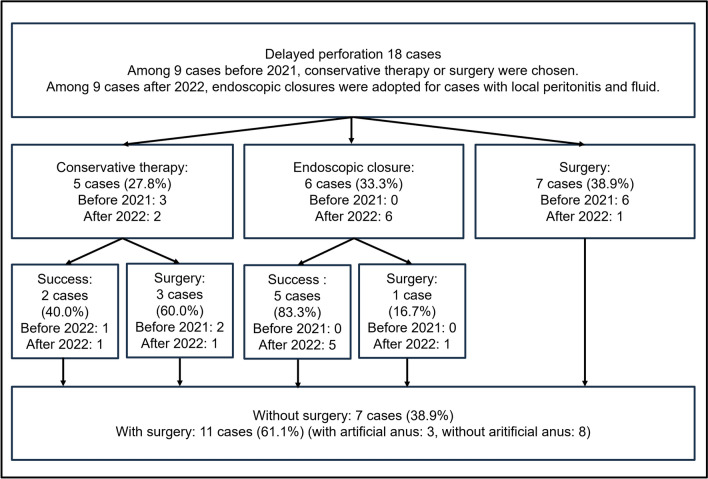
Results: DP occurred in 18 cases, with an incidence rate of 0.39% [95% confidence interval (CI): 0.24-0.62]. The mean tumor size was 49.7 ± 35.7 mm. The rates of right-sided colon lesions and severe fibrosis were observed in 77.8 and 61.2%, respectively. DP occurred on post-procedure day 1 in 55.8% of cases, day 2 in 22.2%, and on day 3 or later in 22.2%. Initial DP management included conservative treatment in five cases (27.8%), endoscopic closure in six (33.3%), and surgery in seven cases (38.9%). Among the six cases managed endoscopically, five (83.3%) were successfully managed without surgery. Finally, surgery was required in 11 cases (61.1%). Multivariate analysis (odds ratio [95%CI]) identified severe fibrosis (4.61 [1.50-14.20], p = 0.007), and long procedure time (1.01 [1.00-1.02], p = 0.042), as significant risk factors for DP, while complete closure was inversely correlated with DP risk (0.12 [0.01-0.96], p = 0.046).
Conclusions: This study identified DP incidence and risk factors after colorectal ESD, with some cases requiring surgery. Endoscopic treatment may prevent surgery.
Keywords: Clipping; Colorectum; Delayed perforation; Endoscopic closure; Endoscopic submucosal dissection.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: Yoshida N and Dohi O received a research grant from Fujifilm Co. Yoshida N received lecture fee from Fujifilm. The other authors declare no conflicts of interest. Ethical approval: This study was approved by the ethics committee of Kyoto Prefectural University of Medicine (ERB-C-1704-5, approval data: June 5, 2024) as a partial study of our large-scale retrospective and prospective study and was conducted in accordance with the World Medical Association Declaration of Helsinki. This was a retrospective study and patients’ informed consent was obtained with the option opt-out from participating.
Figures

References
-
- Tanaka S, Kashida H, Saito Y et al. Japan Gastroenterological Endoscopy Society guidelines for colorectal endoscopic submucosal dissection/endoscopic mucosal resection. Dig Endosc. 2020;32:219–239. - PubMed
-
- Draganov PV, Wang AY, Othman MO et al. AGA Institute Clinical Practice Update: Endoscopic Submucosal Dissection in the United States. Clin Gastroenterol Hepatol. 2019;17:16–25. - PubMed
-
- Ferlitsch M, Hassan C, Bisschops R et al. Colorectal polypectomy and endoscopic mucosal resection: European Society of Gastrointestinal Endoscopy (ESGE) Guideline - Update 2024. Endoscopy. 2024;56:516–545. - PubMed
-
- Ritsuno H, Sakamoto N, Osada T et al. Prospective clinical trial of traction device-assisted endoscopic submucosal dissection of large superficial colorectal tumors using the S-O clip. Surg Endosc. 2014;28:3143–3149. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
