

Age-associated differences in mucosal and systemic host responses to SARS-CoV-2 infection
- PMID: 40064870
- PMCID: PMC11894178
- DOI: 10.1038/s41467-025-57655-3
Age-associated differences in mucosal and systemic host responses to SARS-CoV-2 infection
Abstract
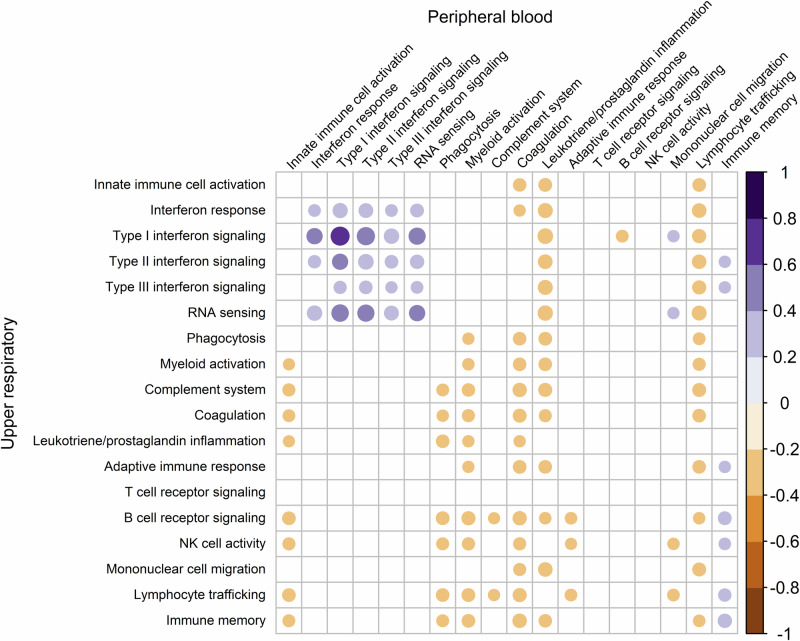
Age is among the strongest risk factors for severe outcomes from SARS-CoV-2 infection. Here we describe upper respiratory tract (URT) and peripheral blood transcriptomes of 202 participants (age range of 1 week to 83 years), including 137 non-hospitalized individuals with mild SARS-CoV-2 infection and 65 healthy individuals. Among healthy children and adolescents, younger age is associated with higher URT expression of innate and adaptive immune pathways. SARS-CoV-2 infection induces broad upregulation of URT innate and adaptive immune responses among children and adolescents. Peripheral blood responses among SARS-CoV-2-infected children and adolescents are dominated by interferon pathways, while upregulation of myeloid activation, inflammatory, and coagulation pathways is observed only in adults. Among SARS-CoV-2-infected individuals, fever is associated with blunted URT immune responses and more pronounced systemic immune activation. These findings demonstrate that immune responses to SARS-CoV-2 differ across the lifespan, from distinct signatures in childhood and adolescence to age-associated alterations in adults.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: T.W.B. is a consultant for and owns equity in Biomeme, Inc. K.M.W. held a sponsored research project from Moderna Therapeutics, Inc. on immune correlates of congenital CMV infection. C.W.W. is a consultant for and owns equity in Biomeme, Inc. M.S.K. is a consultant for Merck & Co, Inc. and Invivyd. N.A.T. has received research contracts with PDI, Purio, and Basilea as well as consulting for Techspert. A.M. is a consultant for Merck, Pfizer, Moderna, Astra-Zeneca, Enanta, and Sanofi-Pasteur. O.R. has received research grants from the Bill & Melinda Gates Foundation, Merck, and Janssen; fees for participation in advisory boards from Merck, Sanofi-Pasteur, Pfizer, and Moderna; and fees for lectures from Pfizer, AstraZeneca, Merck, and Sanofi-Pasteur. All other authors declare that they have no competing interests.
Figures




References
-
- Centers for Disease Control and Prevention (CDC), United States COVID-19 Cases and Deaths by State over Time (available at https://data.cdc.gov/Case-Surveillance/United-States-COVID-19-Cases-and-... (2024).
-
- CDC, Cases, Data, and SurveillanceCenters for Disease Control and Prevention (available at https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-disc...) (2020).
-
- Centers for Disease Control and Prevention, COVID-NET: COVID-19-associated hospitalization surveillance network (available at https://gis.cdc.gov/grasp/covidnet/COVID19_3.html).
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
