

Individualized PEEP can improve both pulmonary hemodynamics and lung function in acute lung injury
- PMID: 40065461
- PMCID: PMC11892255
- DOI: 10.1186/s13054-025-05325-7
Individualized PEEP can improve both pulmonary hemodynamics and lung function in acute lung injury
Abstract
Rationale: There are several approaches to select the optimal positive end-expiratory pressure (PEEP), resulting in different PEEP levels. The impact of different PEEP settings may extend beyond respiratory mechanics, affecting pulmonary hemodynamics.
Objectives: To compare PEEP levels obtained with three titration strategies-(i) highest respiratory system compliance (CRS), (ii) electrical impedance tomography (EIT) crossing point; (iii) positive end-expiratory transpulmonary pressure (PL)-in terms of regional respiratory mechanics and pulmonary hemodynamics.
Methods: Experimental studies in two porcine models of acute lung injury: (I) bilateral injury induced in both lungs, generating a highly recruitable model (n = 37); (II) asymmetrical injury, generating a poorly recruitable model (n = 13). In all experiments, a decremental PEEP titration was performed monitoring PL, EIT (collapse, overdistention, and regional ventilation), respiratory mechanics, and pulmonary and systemic hemodynamics.
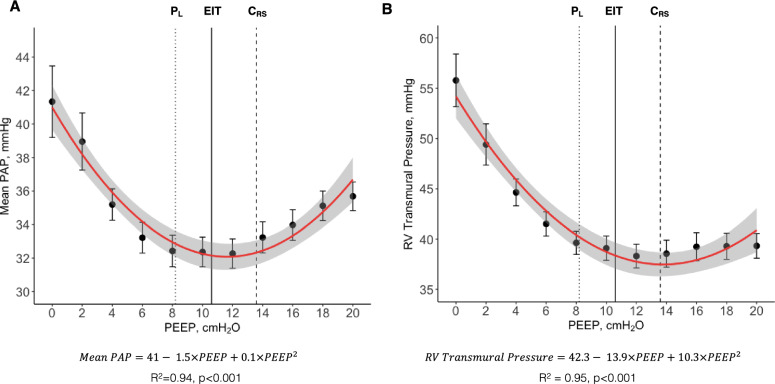
Measurements and main results: PEEP titration methods resulted in different levels of median optimal PEEP in bilateral lung injury: 14(12-14) cmH2O for CRS, 11(10-12) cmH2O for EIT, and 8(8-10) cmH2O for PL, p < 0.001. Differences were less pronounced in asymmetrical lung injury. PEEP had a quadratic U-shape relationship with pulmonary artery pressure (R2 = 0.94, p < 0.001), right-ventricular systolic transmural pressure, and pulmonary vascular resistance. Minimum values of pulmonary vascular resistance were found around individualized PEEP, when ventilation distribution and pulmonary circulation were simultaneously optimized.
Conclusions: In porcine models of acute lung injury with variable lung recruitability, both low and high levels of PEEP can impair pulmonary hemodynamics. Optimized ventilation and hemodynamics can be obtained simultaneously at PEEP levels individualized based on respiratory mechanics, especially by EIT and esophageal pressure.
Keywords: Acute lung injury; Mechanical ventilation; Positive end-expiratory pressure; Pulmonary hemodynamics; Pulmonary vascular resistance.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: The authors declare no competing interests. Ethical approval and consent to participate: The animal study protocol was approved by the Animal Care Committee of the Peter Gilgan Centre for Research and Learning (PGRLC) at The Hospital for Sick Children – SickKids, reference number 1000058058. Consent for publication: Not applicable.
Figures






References
-
- Slutsky AS, Ranieri VM. Ventilator-induced lung injury. N Engl J Med. 2013;369:2126–36. - PubMed
-
- Pham T, Rubenfeld GD. Fifty years of research in ards the epidemiology of acute respiratory distress syndrome a 50th birthday review. Am J Respir Crit Care Med. 2017;195:860–70. - PubMed
-
- Henderson WR, Chen L, Amato MBP, Brochard LJ. Fifty years of research in ARDS respiratory mechanics in acute respiratory distress syndrome. Am J Respir Crit Care Med. 2017;196:822–33. - PubMed
-
- Sousa MLA, Katira BH, Bouch S, Hsing V, Engelberts D, Amato M, et al. Limiting overdistention or collapse when mechanically ventilating injured lungs: a randomized study in a porcine model. Am J Respir Crit Care Med. 2024. 10.1164/rccm.202310-1895OC. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
