

Novel predictors of infection-related rehospitalization in older patients with heart failure in Japan
- PMID: 40066617
- PMCID: PMC11973016
- DOI: 10.1111/ggi.70019
Novel predictors of infection-related rehospitalization in older patients with heart failure in Japan
Abstract
Aim: Rehospitalization of patients with heart failure (HF) incurs high health care costs and increased mortality. Infection-related rehospitalizations in patients with HF occur frequently, and the risk increases with age. This study aimed to identify the factors associated with infection-related rehospitalizations in older patients with HF.
Methods: Demographic, clinical, and pharmacological data from 1061 patients with acute HF who were enrolled in the Kochi Registry of Subjects With Acute Decompensated Heart Failure (Kochi YOSACOI study) were analyzed. Additionally, a machine learning approach was applied in addition to the traditional statistical analysis model. Of the patients hospitalized for HF, 729 were ultimately analyzed.
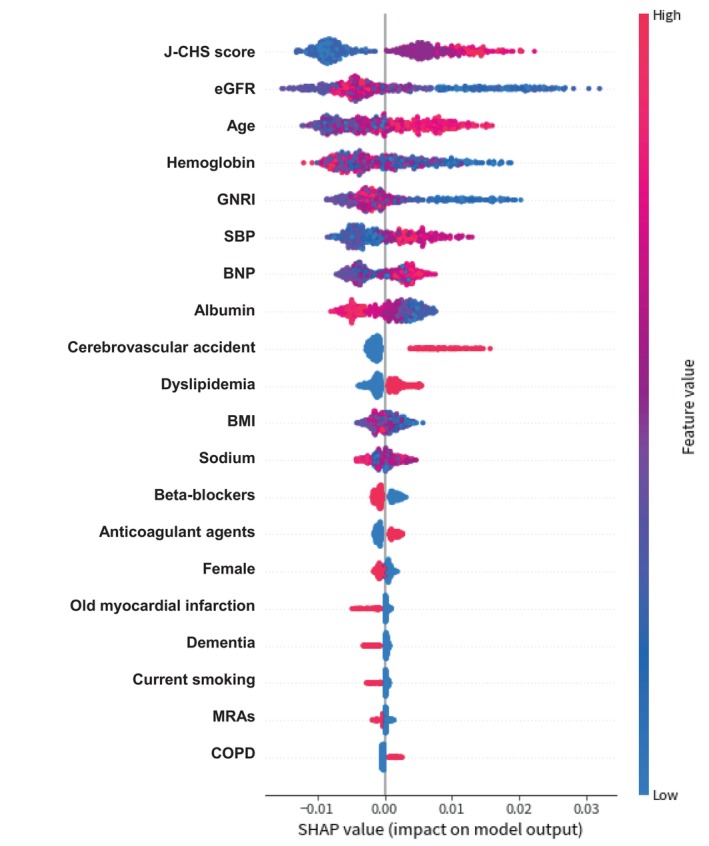
Results: During the 2-year postdischarge follow-up period, 121 (17%) patients were readmitted for infections. Logistic regression analysis identified a Japanese Cardiovascular Health Study (J-CHS) score of ≥3 (odds ratio, 1.83 [95% confidence interval, 1.18-2.83]; P = 0.007) at discharge as a key factor for infection-related rehospitalizations. Machine learning models confirmed that a higher J-CHS score and lower estimated glomerular filtration rate (eGFR) increased the risk of infection-related rehospitalizations. Decision tree analysis classified the risk into high (J-CHS score ≥3), medium (J-CHS score <3; eGFR ≤35.0) and low (J-CHS score <3; eGFR >35.0) groups.
Conclusions: Infection-related rehospitalizations occur in older patients with HF and are associated with frailty and eGFR. These findings provide valuable insights for health care providers to better manage the risk of infection-related rehospitalizations in older patients with HF, potentially improving patient outcomes. Geriatr Gerontol Int 2025; 25: 543-552.
Keywords: J‐CHS score; decision tree; frail; heart failure; infection‐related rehospitalization.
© 2025 The Author(s). Geriatrics & Gerontology International published by John Wiley & Sons Australia, Ltd on behalf of Japan Geriatrics Society.
Figures


References
-
- Redfield MM. Heart failure—an epidemic of uncertain proportions. N Engl J Med 2002; 347: 1442–1444. - PubMed
-
- Tsao CW, Aday AW, Almarzooq ZI et al. Heart disease and stroke statistics‐2023 update: a report from the American Heart Association. Circulation 2023; 147: e93–e621. - PubMed
-
- Ambrosy AP, Fonarow GC, Butler J et al. The global health and economic burden of hospitalizations for heart failure: lessons learned from hospitalized heart failure registries. J Am Coll Cardiol 2014; 63: 1123–1133. - PubMed
-
- Farré N, Vela E, Clèries M et al. Medical resource use and expenditure in patients with chronic heart failure: a population‐based analysis of 88 195 patients. Eur J Heart Fail 2016; 18: 1132–1140. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
