

Extended pharmacological thromboprophylaxis and clinically relevant venous thromboembolism after major abdominal and pelvic surgery: international, prospective, propensity score-weighted cohort study
- PMID: 40067192
- PMCID: PMC11894929
- DOI: 10.1093/bjs/znaf005
Extended pharmacological thromboprophylaxis and clinically relevant venous thromboembolism after major abdominal and pelvic surgery: international, prospective, propensity score-weighted cohort study
Abstract
Background: There is low-certainty evidence on the impact of extended pharmacological prophylaxis on venous thromboembolism-associated morbidity and mortality. The aim of this study was to determine the efficacy and safety of extended prophylaxis after major abdominopelvic surgery for the prevention of clinically relevant venous thromboembolism after hospital discharge.
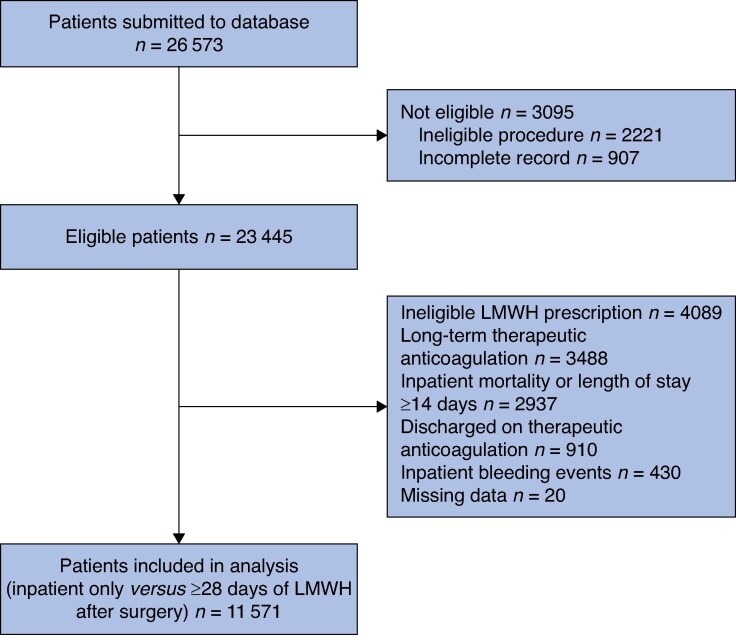
Methods: CArdiovaSCulAr outcomes after major abDominal surgEry (CASCADE) was a prospective, international, cohort study into which consecutive adult patients undergoing major abdominopelvic surgery were enrolled (January-May 2022). Extended prophylaxis was considered at least 28 days of anticoagulant prescription after surgery. The primary efficacy outcome was clinically relevant venous thromboembolism and the primary safety outcome was clinically relevant bleeding within 30 days after surgery (European Medicines Agency definitions). The independent association of these outcomes with extended prophylaxis was explored using mixed-effects logistic regression and propensity score weighting.
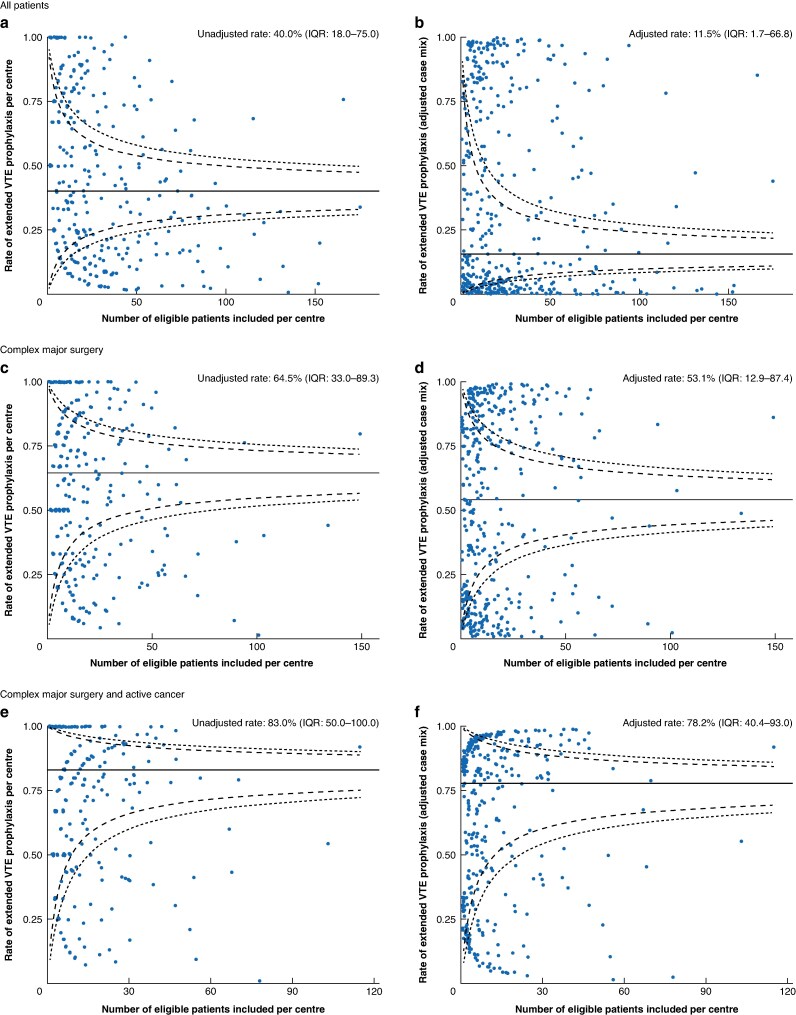
Results: A total of 11 571 patients (median age of 58.0 years; 6399 (55.3%) women) from 29 countries were included. The extended prophylaxis prescription rate was 31.7% (3670 patients). The post-discharge venous thromboembolism and bleeding rates were 0.1% (12 patients) and 0.7% (85 patients) respectively. After weighting, extended prophylaxis was not significantly associated with increased bleeding risk (OR 1.07 (95% c.i. 0.64 to 1.81); P = 0.792) or decreased venous thromboembolism incidence, both in the overall cohort (OR 1.13 (95% c.i. 0.33 to 3.90); P = 0.848) and in a subgroup analysis of patients undergoing complex major surgery and with active cancer (OR: 1.36 (95% c.i. 0.33 to 5.57); P = 0.669).
Conclusion: In modern practice, the incidence of postoperative venous thromboembolism is low. Extended prophylaxis appears safe, yet the clinical efficacy remains uncertain. Further work is required to define patients who stand to benefit.
Plain language summary
Blood clots are a possible complication after major surgery. These can be very serious. If they form in the legs, they can cause swelling and pain. If they travel to the lungs, they can cause breathlessness or chest pain, and can be life-threatening. Injections of blood thinners (heparin) under the skin for at least 28 days after surgery can reduce the total number of blood clots. However, only some blood clots cause symptoms and it is unclear whether the heparin injections can reduce the number of symptomatic blood clots. In this study, the authors wanted to look at whether the injections can reduce the number of symptomatic blood clots, without increasing the risk of bleeding, after surgery. This was a large, international study that collected data on adult patients having major abdominal and pelvic surgery. The authors used robust statistical methods to compare patients who received or did not receive the heparin injections. This study included 11 571 patients from 29 countries. Around one-third received the heparin injections for at least 28 days. Only 12 people developed clots after surgery. The authors did not find that the injections reduced the likelihood of developing symptomatic blood clots. The injections did not increase the risk of bleeding. The findings suggest that 28 days of heparin injections might not be useful for all patients having major abdominal or pelvic surgery. The authors’ opinion is that these should be reserved for those that have a higher risk of developing blood clots.
© The Author(s) 2025. Published by Oxford University Press on behalf of BJS Foundation Ltd.
Figures
References
-
- Lavikainen LI, Guyatt GH, Sallinen VJ, Karanicolas PJ, Couban RJ, Singh T et al. Systematic reviews and meta-analyses of the procedure-specific risks of thrombosis and bleeding in general abdominal, colorectal, upper gastrointestinal, and hepatopancreatobiliary surgery. Ann Surg 2024;279:213–225 - PMC - PubMed
-
- Gould MK, Garcia DA, Wren SM, Karanicolas PJ, Arcelus JI, Heit JA et al. Prevention of VTE in nonorthopedic surgical patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012; 141(Suppl): e227S–e277S - PMC - PubMed
