

Dynamic HER2-low status among patients with triple negative breast cancer (TNBC) and the impact of repeat biopsies
- PMID: 40069204
- PMCID: PMC11897376
- DOI: 10.1038/s41523-025-00741-y
Dynamic HER2-low status among patients with triple negative breast cancer (TNBC) and the impact of repeat biopsies
Abstract
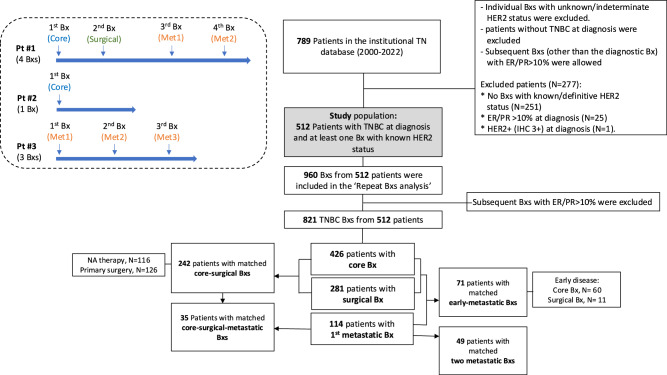
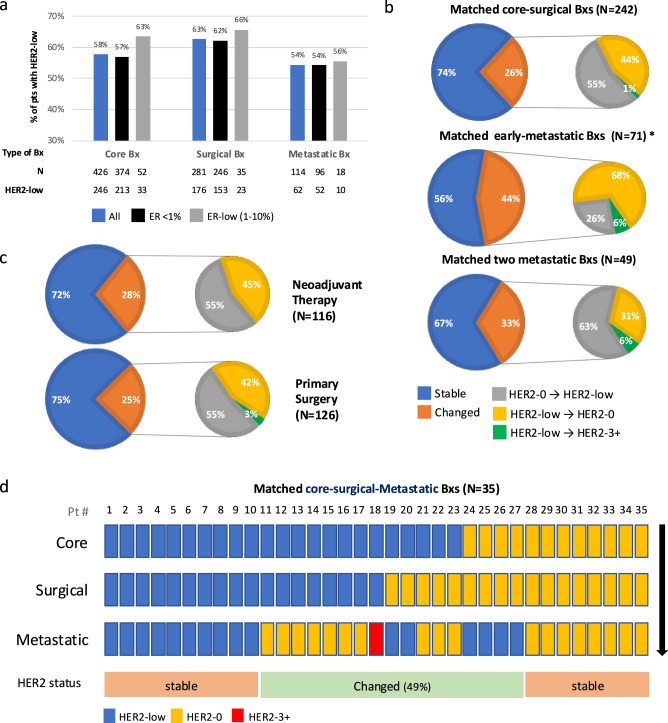
Trastuzumab deruxtecan (T-DXd) is approved for HER2-low (HER2 immunohistochemistry (IHC)1+ or 2+ with non-amplified in situ hybridization (ISH)), but not HER2-0 (IHC 0) metastatic breast cancer. The impact of repeat biopsies (Bxs) in identifying new potential candidates with triple negative breast cancer (TNBC) for T-DXd treatment remains unknown. 512 consecutive patients with TNBC at diagnosis were included in the study cohort. Bxs were categorized as core, surgical, or metastatic based on the timing and method of biopsy (Bx) acquisition, and the total number of Bxs was determined for each patient. Additionally, matched biopsies were identified, and the rate of discordance in HER2 status was calculated. The proportion of patients with at least one HER2-low result increased as the number of successive Bxs increased [59%, 73%, 83%, 83%, and 100% when 1 (196 patients), 2 (231 patients), 3 (48 patients), 4 (29 patients), and ≥ 5 (8 patients) Bxs were obtained, respectively]. Among patients without a prior HER2-low result, approximately one-third demonstrated HER2-low status with each additional successive Bx. HER2 status exhibited variability between matched Bxs, with observed discordance rates of 26%, 44%, and 33% between matched core-surgical, early-metastatic, and two metastatic matched Bxs, respectively. Our findings indicate that HER2 status can vary between different Bxs taken during the disease course of patients with TNBC with the highest discordance rate observed between the primary and metastatic Bxs. For patients with metastastic HER2-0 TNBC, repeat Bxs can increase the chance of obtaining a HER2-low result, thereby offering patients a promising therapeutic option.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: No funding was provided for this study. Individual disclosures for co-authors are as noted below:Y. B reports honoraria for lectures from Stemline, Lilly, Roche, Gilead, Pfizer, Novartis; and consulting/advisory role for Lilly, Novartis. L.W.E reports consulting/advisory role for Mersana Therapeutics, Kisoji Biotech and Astra Zeneca. L.M.S reports consultant/advisory role for Novartis, Daiichi Pharma, Astra Zeneca, Eli Lilly, Precede, Seagen; institutional research support from Merck, Genentech, Gilead, Eli Lilly, Astra Zeneca; and travel support from Eli Lilly. S.A.W reports consulting/advisory role for Foundation Medicine, Veracyte, Hologic, Eli Lilly, Biovica, Pfizer/Arvinas, Puma Biotechnology, Novartis, AstraZeneca, Genentech, Regor Therapeutics, Menarini; education/speaking fees from Eli Lilly, Guardant Health, 2ndMD; and institutional research support from Genentech, Eli Lilly, Pfizer/Arvinas, Nuvation Bio, Regor Therapeutics, Sermonix. N.V reports research funding to the institution (MGH) from Merck, Daehwa, Novartis, Pfizer, Radius, Stemline, Ellipses; and advisory board participation (all ended) for AbbVie, OncoSec, Gilead, Aadi, TerSera, Novartis, IDEOlogy Health. A.B. reports consulting or advisory Role for Pfizer, Novartis, Genentech, Merck & Co., Radius Health, Immunomedics/Gilead, Sanofi, Daiichi Pharma/AstraZeneca, Phillips, Eli Lilly and Foundation Medicine and research/grant (to institution) from Genentech, Novartis, Pfizer, Merck & Co., Sanofi, Radius Health, Immunomedics/Gilead, Daiichi Pharma/AstraZeneca and Eli Lilly. The remaining authors declare no competing interests.
Figures

References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
