

Management of acute coronary syndrome in resource-limited set up: a summary of 4-year review of two hospitals in Ethiopia
- PMID: 40071230
- PMCID: PMC11893824
- DOI: 10.3389/fcvm.2025.1520899
Management of acute coronary syndrome in resource-limited set up: a summary of 4-year review of two hospitals in Ethiopia
Abstract
Introduction: Acute coronary syndrome refers to a group of diseases characterized by sudden, decreased blood supply to the heart muscle that results in cell death, also known as acute myocardial infarction. This results in severe chest pain or discomfort, with the subsequent release of cardiac biomarkers, and alterations in the electrocardiogram. It can cause diminished heart function and mortality if not treated properly with suitable measures. Despite the fact that percutaneous coronary intervention is the standard of care in one subset of acute coronary syndrome, significant number of patients were treated medically due to the limited service in the setting. The purpose of this study was to look at the patterns of acute coronary syndrome (ACS), as well as the management and outcomes of these patients in two Ethiopian tertiary institutions.
Methods: A four-year retrospective study was undertaken on 308 patients with acute coronary syndrome, at two tertiary hospitals located in Ethiopia's capital-Addis Ababa.
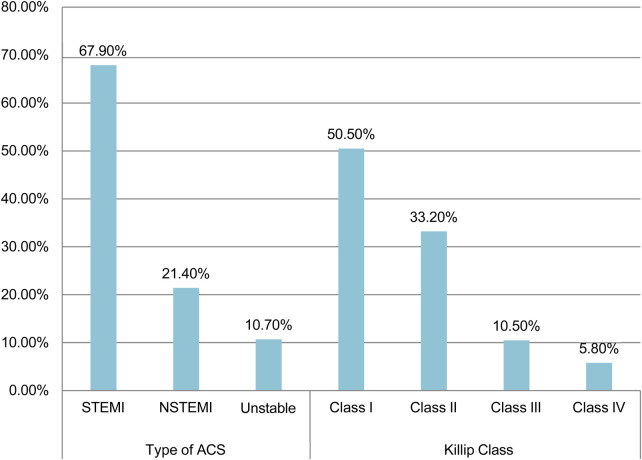
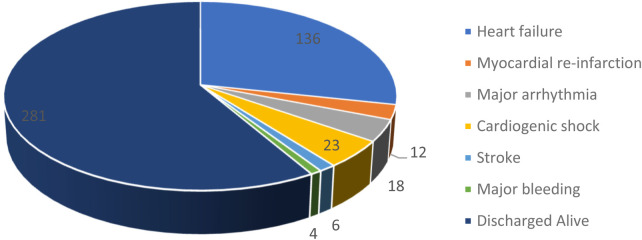
Results and discussion: Of the 308 patients 72.4% were male, with the average age of 56.3 ± 13.5 years. Hypertension and diabetes were the two most common risk factors identified. The average time to present to the emergency room after symptom onset was 3.7 (SD ± 3.2) days. The majority of patients (67.9%) have been diagnosed with ST- Elevated Myocardial Infarction and were classified as Killip class I. Percutaneous Coronary Intervention was performed for 12.3% of patients, with the remaining receiving medical care. The average hospital stay was 8.51 (SD ± 7.2) days while In-hospital mortality was 8.8%. Tachycardia of >140 (AOR = 7.50, 95% CI: 1.36, 41.57), any degree of left ventricular dysfunction, Killip class IV (AOR = 6.03, 95% CI: 1.27, 28.61), and non-initiation of betablockers (AOR = 0.17,95% CI: 0.05, 0.63) were significantly associated with increased in-hospital mortality.
Keywords: Ethiopia; PCI; STEMI; acute coronary syndrome; beta-blockers; heart failure; klipp class.
© 2025 Kebede, Woyimo, Geleta, Chiri, Asefa and Tukeni.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
-
- Amsterdam EA, Wenger NK, Brindis RG, Casey DE, Ganiats TG, Holmes DR, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: executive summary: a report of the American College of Cardiology/American Heart Association task force on practice guidelines. J Am Coll Cardiol. (2014) 64(24):e139–228. 10.1016/j.jacc.2014.09.016 - DOI - PubMed
-
- Wilkins E, Wilson L, Wickramasinghe K, Bhatnagar P, Leal J, Luengo-Fernandez R, et al. European Cardiovascular Disease Statistics 2017. 5th ed. Brussels: European Heart Network; (2017):1–72.
LinkOut - more resources
Full Text Sources
Miscellaneous