

Multi-level barriers to equitable postpartum permanent contraception
- PMID: 40072008
- PMCID: PMC11905033
- DOI: 10.1177/17455057251325977
Multi-level barriers to equitable postpartum permanent contraception
Abstract
Background: There are several barriers to fulfillment of desired postpartum permanent contraception (PC). Prior research has primarily focused on the federal Medicaid sterilization policy as a barrier to PC; however, other barriers need to be examined.
Objectives: To explore the levels and intersections of barriers to postpartum PC that exist external to the Medicaid policy.
Design: We interviewed postpartum people with a documented desire for PC and their delivering obstetrician-gynecologist (OB-GYN) at four hospitals in the United States in 2022-2023.
Methods: We used rapid qualitative analysis to create initial key themes and sub-themes, which we further refined using thematic analysis to explore barriers to postpartum PC.
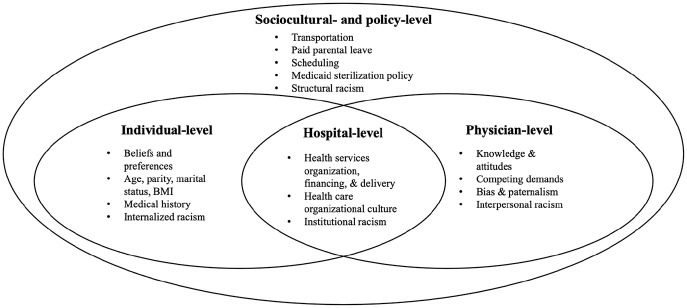
Results: We interviewed 81 postpartum people and 67 OB-GYNs. Barriers were identified across four levels: clinical, physician, hospital, and sociocultural. At the clinical level, participants commented on how they believed individual patient characteristics and medical history can prevent PC fulfillment prior to discharge. At the physician level, participants discussed young age, low parity, and marital status as reasons clinicians decline to provide desired PC. At the hospital level, OB-GYNs described difficulties with scheduling and staffing, and patients described a lack of PC prioritization. At the sociocultural level, participants mentioned numerous barriers to fulfillment of interval PC including finding childcare, getting appointments scheduled quickly, and transportation.
Conclusion: Improving access to postpartum PC should be focused within and across all levels of health disparity determinants. In the cases where immediate PC is not accessible, interventions should be formulated across levels to allow timely access to interval PC. As policy reform alone will not eliminate all barriers to postpartum PC, a multi-level approach to alleviating barriers is required.
Keywords: Kilbourne framework; health determinants; multi-level barriers; permanent contraception; reproductive health.
Plain language summary
Multi-level barriers to equitable postpartum permanent contraceptionWhy was the study done? Prior research indicates that the federal Medicaid sterilization policy poses as a barrier to permanent contraception fulfillment. Only 53% of patients with Medicaid receive their desired postpartum permanent contraception, compared to 70% of patients with private insurance. Prior research has primarily focused on the federal Medicaid sterilization policy as a barrier to permanent contraception; however, other barriers and their intersections warrant examination. What did the researchers do? The research team explored the levels and intersections of barriers to permanent contraception fulfillment that exist external to the Medicaid policy. They conducted semi-structured, qualitative interviews with postpartum patients with a documented desire for permanent contraception and their delivering obstetrician–gynecologist. What did the researchers find? Barriers to postpartum permanent contraception fulfillment are prevalent across four overarching levels: clinical, physician, hospital, and sociocultural. At the clinical level, individual patient characteristics and medical histories may prevent permanent contraception fulfillment. At the physician level, cutoffs around age, marital status, and parity may prompt physicians to decline provision. At the hospital level, staffing and scheduling issues complicate fulfillment prior to discharge. Lastly, at the sociocultural level, difficulty with childcare, transportation, and appointment scheduling may prevent interval permanent contraception fulfillment. What do the findings mean? Public health interventions should be developed across each level of determinants to improve access to permanent contraception and eliminate inequities.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Fulfillment of Desired Postpartum Permanent Contraception: a Health Disparities Issue.Reprod Sci. 2022 Sep;29(9):2620-2624. doi: 10.1007/s43032-022-00912-3. Epub 2022 Jun 17. Reprod Sci. 2022. PMID: 35713848 Free PMC article.
-
Obstetrician-Gynecologist Perspectives and Counseling Practices on the U.S. Medicaid Waiting Period for Permanent Contraception.Womens Health Issues. 2025 Mar-Apr;35(2):83-88. doi: 10.1016/j.whi.2025.01.002. Epub 2025 Feb 17. Womens Health Issues. 2025. PMID: 39965989
-
Medicaid and Fulfillment of Postpartum Permanent Contraception Requests.Obstet Gynecol. 2023 May 1;141(5):918-925. doi: 10.1097/AOG.0000000000005130. Epub 2023 Apr 5. Obstet Gynecol. 2023. PMID: 37103533 Free PMC article.
-
Postpartum permanent contraception: updates on policy and access.Curr Opin Obstet Gynecol. 2021 Dec 1;33(6):445-452. doi: 10.1097/GCO.0000000000000750. Curr Opin Obstet Gynecol. 2021. PMID: 34534995 Review.
-
Ethics of a Mandatory Waiting Period for Female Sterilization.Hastings Cent Rep. 2022 Jul;52(4):17-25. doi: 10.1002/hast.1405. Hastings Cent Rep. 2022. PMID: 35993104 Free PMC article. Review.
Cited by
-
Reproductive outcomes of patients with unfulfilled postpartum permanent contraception requests.Womens Health (Lond). 2025 Jan-Dec;21:17455057251356883. doi: 10.1177/17455057251356883. Epub 2025 Jul 28. Womens Health (Lond). 2025. PMID: 40726083 Free PMC article.
References
-
- Daniels K, Abma J. Current Contraceptive Status Among Women Aged 15–49: United States, 2017–2019. NCHS Data Brief No. 388, Report, USA, 2020. - PubMed
-
- No Author. Access to postpartum sterilization: ACOG Committee Opinion, Number 827. Obstet Gynecol 2021; 137(6): e169–e176. - PubMed
-
- Block-Abraham D, Arora KS, Tate D, et al.. Medicaid consent to sterilization forms. Clin Obstet Gynecol 2015; 58(2): 409–417. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
