

Development and evaluation of an automated phenylephrine delivery system by lower limit control for managing intraoperative hypotension
- PMID: 40072565
- PMCID: PMC12103478
- DOI: 10.1007/s00540-025-03476-z
Development and evaluation of an automated phenylephrine delivery system by lower limit control for managing intraoperative hypotension
Abstract
Purpose: In this study, we aimed to develop and evaluate an automated phenylephrine delivery system by lower limit control for the management of intraoperative hypotension, assessing its efficacy in maintaining adequate blood pressure levels.
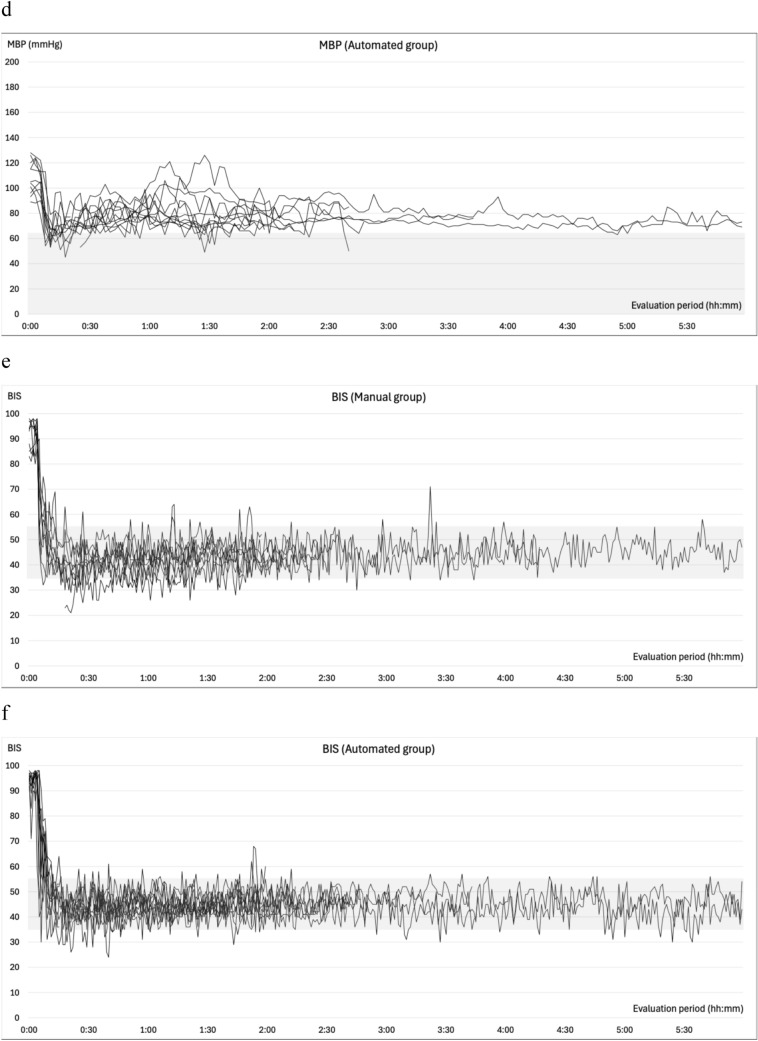
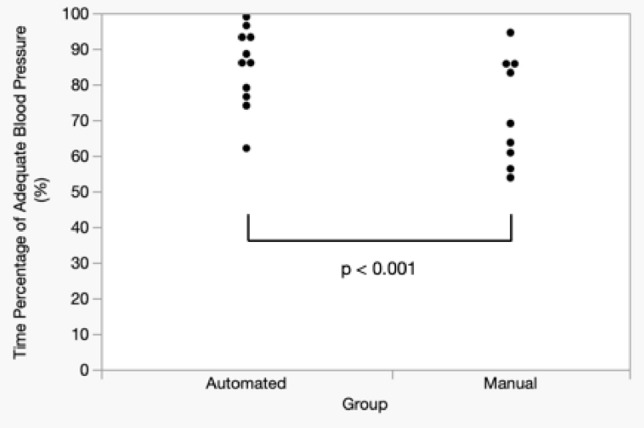
Methods: Twenty patients undergoing surgery with anticipated blood pressure fluctuations were enrolled in this study. Patients were randomly assigned to two groups. Noninvasive blood pressure (NIBP) was measured at 2.5-min intervals using an upper arm cuff. In the automated group, phenylephrine administration was governed by an automated system that delivered bolus doses and adjusted the continuous infusion rate when mean blood pressure (MBP) dropped below 65 mmHg. In the manual group, phenylephrine administration was initiated by the attending anesthesiologist under the same MBP threshold. Propofol, remifentanil, and rocuronium were administered via the automated delivery system for total intravenous anesthesia, to minimize hemodynamic variability between groups. The primary end point was the percentage of time during which MBP remained above 65 mmHg and systolic blood pressure below 140 mmHg, measured from the initiation to the cessation of intravenous anesthesia and assessed using a non-inferiority test.
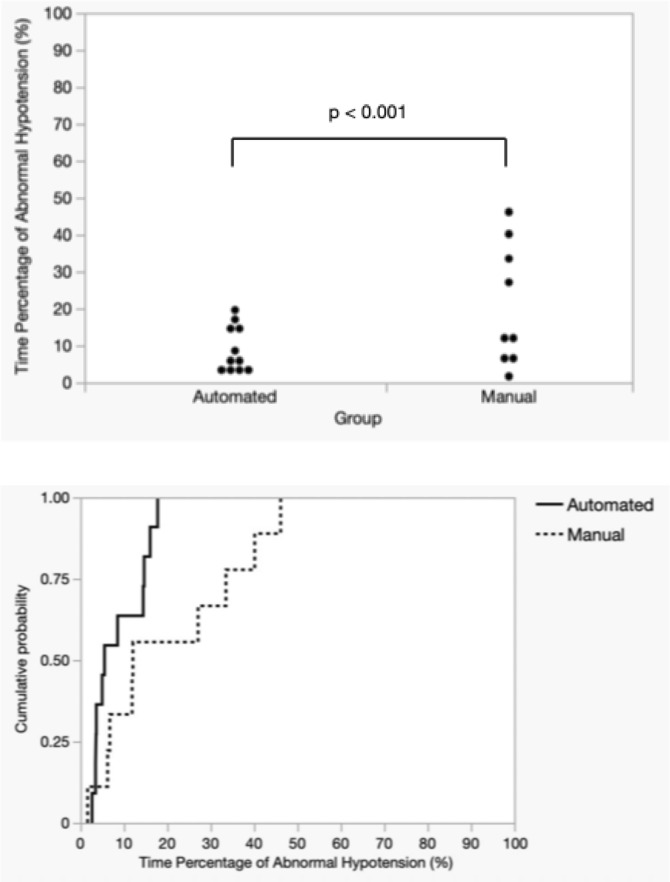
Results: The automated group adequately maintained blood pressure within the target range for 84.53% of the time, compared to 72.45% in the manual group, confirming statistical non-inferiority (p < 0.001).
Conclusion: This system effectively managed intraoperative hypotension using intermittent NIBP measurements, which are more feasible in clinical practice. Despite relying on less frequent and lower-resolution blood pressure data, it demonstrated efficacy comparable to anesthesiologist-led management, indicating its potential for broader clinical application.
Keywords: Automated drug delivery system; Intraoperative hypotension; Lower limit control; Noninvasive blood pressure measurement; Phenylephrine.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: Osamu Nagata holds a patent on the automated delivery system for intravenous anesthetics; Emi Morinushi, Aya Kuroyanagi, and Fumiyo Yasuma have no conflicts of interest.
Figures









Comment in
-
Letter to the article by Nagata et al.J Anesth. 2025 Aug 18. doi: 10.1007/s00540-025-03565-z. Online ahead of print. J Anesth. 2025. PMID: 40824289 No abstract available.
References
-
- Cardenas-Garcia J, Schaub KF, Belchikov YG, Narasimhan M, Koenig SJ, Mayo PH. Safety of peripheral intravenous administration of vasoactive medication. J Hosp Med. 2015;10:581–5. - PubMed
-
- Ngan Kee WD, Tam YH, Khaw KS, Ng FF, Critchley LA, Karmakar MK. Closed-loop feedback computer-controlled infusion of phenylephrine for maintaining blood pressure during spinal anaesthesia for caesarean section: a preliminary descriptive study. Anaesthesia. 2007;62:1251–6. - PubMed
-
- Joosten A, Rinehart J, Van der Linden P, Alexander B, Penna C, De Montblanc J, Cannesson M, Vincent JL, Vicaut E, Duranteau J. Computer-assisted individualized hemodynamic management reduces intraoperative hypotension in intermediate- and high-risk surgery: a randomized controlled trial. Anesthesiology. 2021;135:258–72. - PMC - PubMed
-
- Nagata O, Matsuki Y, Matsuda S, Hazama K, Fukunaga S, Nakatsuka H, Yasuma F, Maehara Y, Fujioka S, Tajima K, Kondo I, Ginoza I, Hayashi M, Kakinohana M, Shigemi K. Anesthesia management via an automated control system for propofol, remifentanil, and rocuronium compared to management by anesthesiologists: an investigator-initiated study. J Clin Med. 2023;12:6611. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
