

Soft tissue manipulation enhances recovery of muscle mass in a disuse model of sarcopenia
- PMID: 40073288
- PMCID: PMC12353430
- DOI: 10.1515/jom-2024-0247
Soft tissue manipulation enhances recovery of muscle mass in a disuse model of sarcopenia
Abstract
Context: Sarcopenia is a disease characterized by low muscle mass and function that places individuals at greater risk of disability, loss of independence, and death. Current therapies include addressing underlying performance issues, resistance training, and/or nutritional strategies. However, these approaches have significant limitations, and chronic inflammation associated with sarcopenia may blunt the anabolic response to exercise and nutrition. This presents an unmet need for treatment strategies that promote gains in muscle function. One such possibility is soft tissue manipulation (STM), which is a noninvasive, nonpharmacological mechanotherapy employed by osteopathic physicians, physiotherapists, and massage therapists, wherein soft tissues are subjected to mechanical forces delivered by hand or by an instrument. However, the molecular effects of STM in sarcopenia remain largely unknown.
Objectives: In the present study, we utilized a rat model of sarcopenia due to disuse atrophy and examined the effects of STM on recovery of muscle mass and regulation of pro-/anti-inflammatory cytokines.
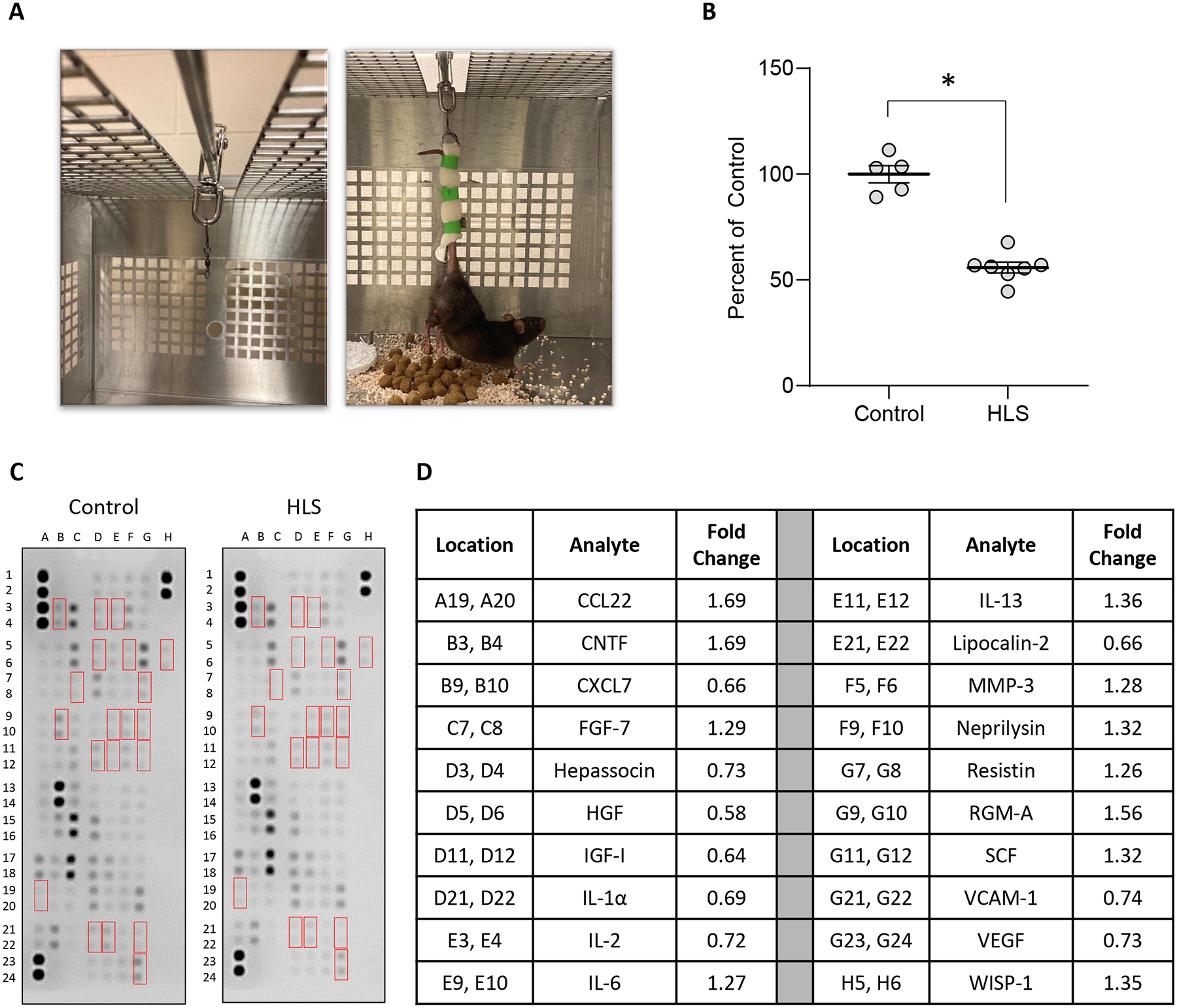
Methods: Ten-week-old male Brown Norway rats were subjected to 2-week hindlimb suspension (HLS) and then allowed to re-ambulate for 8 days with or without instrument-assisted soft tissue manipulation (IASTM) applied to the right hindlimb. Muscle weights were determined for treated and nontreated hindlimbs, and membrane-based cytokine arrays were performed on treated tissue and serum.
Results: Following suspension, IASTM enhanced the effectiveness of re-ambulation (Re-A) on muscle mass recovery in both treated and contralateral limbs. This was associated with changes in numerous cytokines in treated skeletal muscle and sera. Several factors we observe to be regulated were also shown to be regulated by STM in other studies, including ciliary neurotrophic factor (CNTF), IL-1β, IL-2, IL-3, IL-13, ICAM-1, and tumor necrosis factor alpha (TNF-α), whereas others are reported for the first time.
Conclusions: Our study adds further support for the role of manual therapy in musculoskeletal health and details molecular-level effects in both target tissue and circulation. STM may hold promise for recovering muscle mass and function related in conditions of atrophy such as age-related sarcopenia.
Keywords: inflammation; manual therapy; muscle atrophy; rehabilitation; sarcopenia; soft tissue.
© 2025 the author(s), published by De Gruyter, Berlin/Boston.
Conflict of interest statement
Figures





References
-
- Papadopoulou SK, Tsintavis P, Potsaki P, Papandreou D. Differences in the prevalence of sarcopenia in community-dwelling, nursing home and hospitalized individuals. A systematic review and meta-analysis. J Nutr Health Aging 2020;24:83–90. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous