

TGFβ links EBV to multisystem inflammatory syndrome in children
- PMID: 40074901
- PMCID: PMC12003184
- DOI: 10.1038/s41586-025-08697-6
TGFβ links EBV to multisystem inflammatory syndrome in children
Abstract
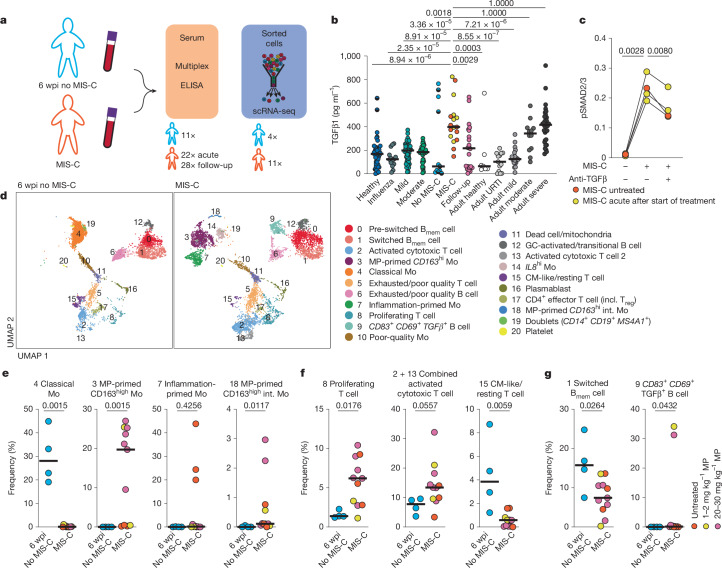
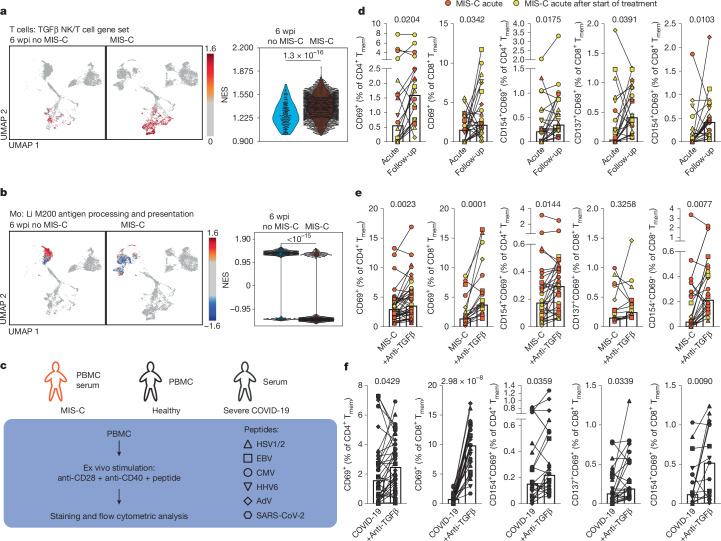
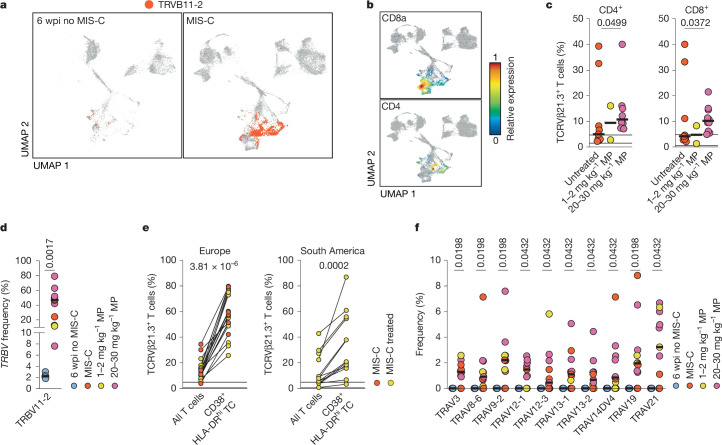
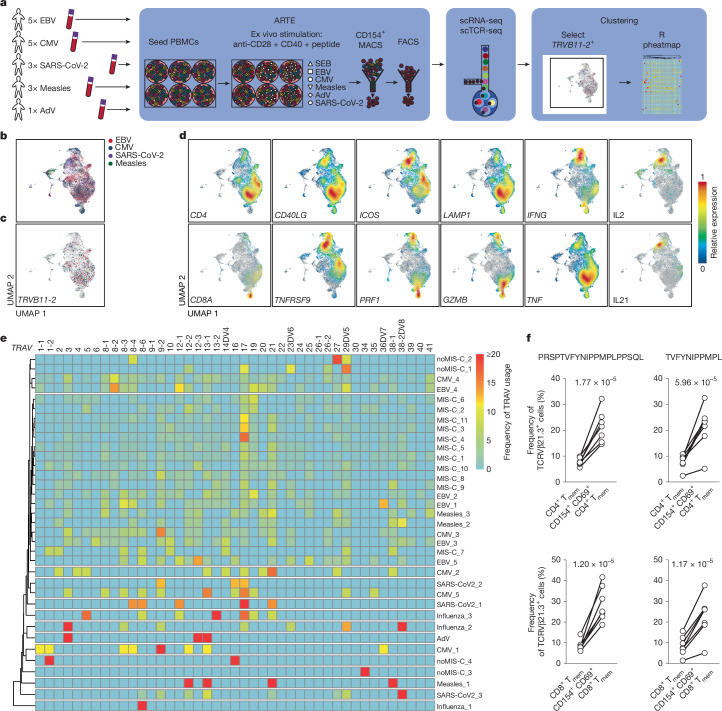
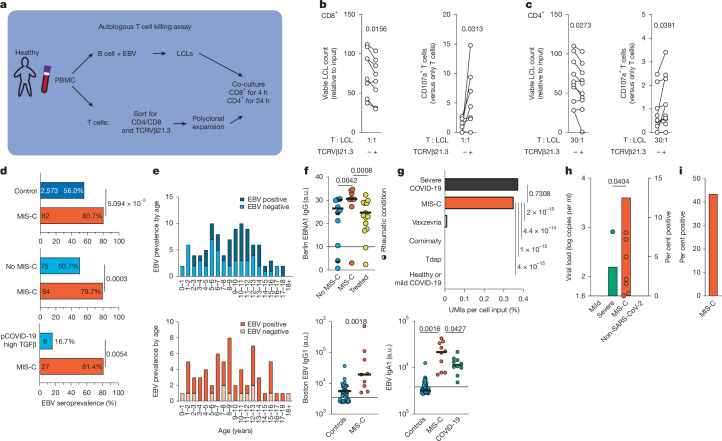
In a subset of children and adolescents, SARS-CoV-2 infection induces a severe acute hyperinflammatory shock1 termed multisystem inflammatory syndrome in children (MIS-C) at four to eight weeks after infection. MIS-C is characterized by a specific T cell expansion2 and systemic hyperinflammation3. The pathogenesis of MIS-C remains largely unknown. Here we show that acute MIS-C is characterized by impaired reactivation of virus-reactive memory T cells, which depends on increased serum levels of the cytokine TGFβ resembling those that occur during severe COVID-19 (refs. 4,5). This functional impairment in T cell reactivity is accompanied by the presence of TGFβ-response signatures in T cells, B cells and monocytes along with reduced antigen-presentation capabilities of monocytes, and can be reversed by blocking TGFβ. Furthermore, T cell receptor repertoires of patients with MIS-C exhibit expansion of T cells expressing TCRVβ21.3, resembling Epstein-Barr virus (EBV)-reactive T cell clones capable of eliminating EBV-infected B cells. Additionally, serum TGFβ in patients with MIS-C can trigger EBV reactivation, which is reversible with TGFβ blockade. Clinically, the TGFβ-induced defect in T cell reactivity correlates with a higher EBV seroprevalence in patients with MIS-C compared with age-matched controls, along with the occurrence of EBV reactivation. Our findings establish a connection between SARS-CoV-2 infection and COVID-19 sequelae in children, in which impaired T cell cytotoxicity triggered by TGFβ overproduction leads to EBV reactivation and subsequent hyperinflammation.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: M.-F.M., C.C.G., T.K. and P.D. filed a patent using TGFβ blockade for management of MIS-C and other post-COVID-19 sequelae. S.P. is an employee of bioMérieux. Y.O. received lecture fees from Pfizer on topics unrelated to this article. S.O. received speaker and/or consultancy fees from Novartis and Sobi on topics unrelated to this article. The authors declare no further competing interests.
Figures









References
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
