

Mapping variants in thyroid hormone transporter MCT8 to disease severity by genomic, phenotypic, functional, structural and deep learning integration
- PMID: 40075072
- PMCID: PMC11904026
- DOI: 10.1038/s41467-025-56628-w
Mapping variants in thyroid hormone transporter MCT8 to disease severity by genomic, phenotypic, functional, structural and deep learning integration
Abstract
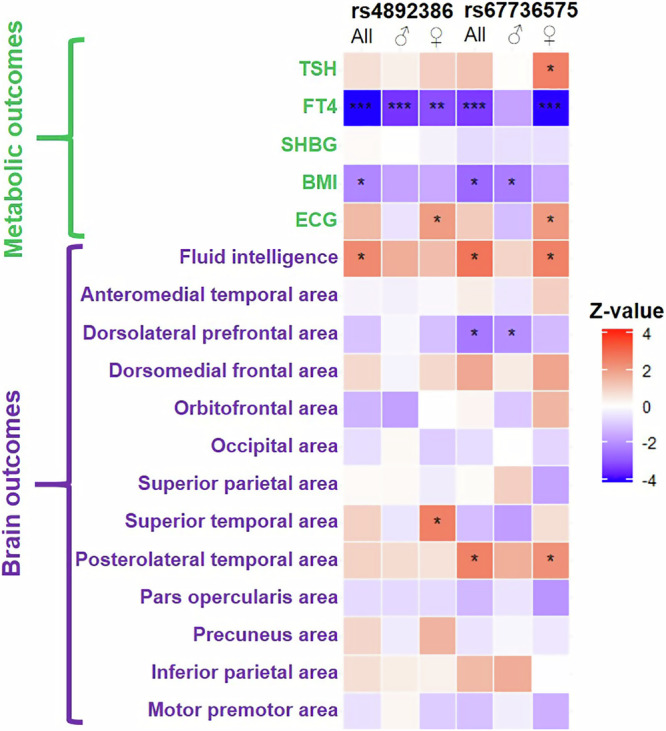
Predicting and quantifying phenotypic consequences of genetic variants in rare disorders is a major challenge, particularly pertinent for 'actionable' genes such as thyroid hormone transporter MCT8 (encoded by the X-linked SLC16A2 gene), where loss-of-function (LoF) variants cause a rare neurodevelopmental and (treatable) metabolic disorder in males. The combination of deep phenotyping data with functional and computational tests and with outcomes in population cohorts, enabled us to: (i) identify the genetic aetiology of divergent clinical phenotypes of MCT8 deficiency with genotype-phenotype relationships present across survival and 24 out of 32 disease features; (ii) demonstrate a mild phenocopy in ~400,000 individuals with common genetic variants in MCT8; (iii) assess therapeutic effectiveness, which did not differ among LoF-categories; (iv) advance structural insights in normal and mutated MCT8 by delineating seven critical functional domains; (v) create a pathogenicity-severity MCT8 variant classifier that accurately predicted pathogenicity (AUC:0.91) and severity (AUC:0.86) for 8151 variants. Our information-dense mapping provides a generalizable approach to advance multiple dimensions of rare genetic disorders.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The Erasmus Medical Center (Rotterdam, Netherlands), which employs SG, FSvG, RBTMS, ELTvdA, SAAvdB, IMvB, MHGD, SL, ALM, MTS, HvT, MdW, RvdW, MCYdW, MEM, MM and WEV receives royalties from Egetis Therapeutics (the manufacturer of Triac). None of the authors will benefit personally from any royalties. Egetis Therapeutics had no influence on the conduct or analysis of this study. The remaining authors declare no competing interests.
Figures





References
-
- Fagerberg, L., Jonasson, K., von Heijne, G., Uhlen, M. & Berglund, L. Prediction of the human membrane proteome. Proteomics10, 1141–1149 (2010). - PubMed
-
- Almeida, J. G., Preto, A. J., Koukos, P. I., Bonvin, A. & Moreira, I. S. Membrane proteins structures: A review on computational modeling tools. Biochim Biophys. Acta Biomembr.1859, 2021–2039 (2017). - PubMed
