

The safety of direct transeptal puncture using a radiofrequency guidewire combined with a 17Fr pulsed field ablation sheath
- PMID: 40075133
- PMCID: PMC11903654
- DOI: 10.1038/s41598-025-88447-w
The safety of direct transeptal puncture using a radiofrequency guidewire combined with a 17Fr pulsed field ablation sheath
Abstract
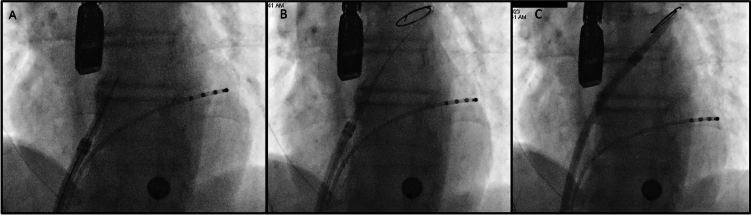
Transseptal puncture (TSP) is widely used in catheter-based cardiac interventions to gain left atrial (LA) access, but its workflow has remained largely unchanged and is still a source of serious complications. Pulsed field ablation (PFA) for pulmonary vein isolation (PVI) has been shown to be at least comparable with radiofrequency ablation (RFA) in terms of safety and efficacy. However, PFA catheter delivery to the LA typically requires a standard TSP and an over the wire sheath exchange which can limit workflow and lengthen procedure time-a shorter procedure time being a proposed advantage of PFA over RFA. This study aimed to evaluate a simplified workflow for direct TSP using the PFA sheath (Faradrive, Boston Scientific). We retrospectively analyzed 166 patients undergoing PVI with PFA in our center. TSP was performed by combining a 16.8F PFA sheath (Faradrive, Boston Scientific) and a RF-guidewire (Versacross, Boston Scientific) as a direct approach without the need over an over-the-wire exchange. The patient population had a mean age of 63.8 ± 11.3 years and was 72.3% male (n = 119/166). TSP was achieved in all patients (n = 166, 100%) without complication. The mean time from groin puncture to LA ablation catheter delivery was 16.2 ± 5.5 min with a mean fluoroscopy time of 15.7 ± 12.7 min. Dilator and sheath crossed the septum with no significant resistance in all cases (n = 168, 100%). The RF-guidewire allowed catheters to be tracked back up to the superior vena cava without exchange in cases where another dropdown was desired to locate a preferred puncture site. The stiffness of the wire provided adequate support to advance all sheaths to the left side regardless of outer diameter. This is the first case series on the use of a RF-guidewire combined with the PFA sheath for TSP. This study proved that an over a RF-powered guidewire TSP directly with 16.8F PFA sheath is feasible, reproducible, and safe. This very simplified workflow eliminates the need for both a rigid metal needle and an over the wire sheath exchange reducing procedure time and complexity, fluoroscopy time and potential related risks.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures


References
-
- Frangieh, A. H. et al. Intracardiac versus transesophageal echocardiography for leD atrial appendage occlusion with watchman. Catheter Cardiovasc. Interv.90(2), 331–338 (2017). - PubMed
-
- Isath, A. et al. Does the use of intracardiac echocardiography during atrial fibrilla_on catheter abla_on improve outcomes and cost? A na_onwide 14-year analysis from 2001 to 2014. J. Interv. Card Electrophysiol.61(3), 461–8 (2021). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
