

Apparent Diffusion Coefficient as an Early Predictive Factor of Local and Overall Response to Treatment with Androgen Deprivation Therapy and Radiotherapy in Patients with Prostate Cancer
- PMID: 40075610
- PMCID: PMC11898613
- DOI: 10.3390/cancers17050762
Apparent Diffusion Coefficient as an Early Predictive Factor of Local and Overall Response to Treatment with Androgen Deprivation Therapy and Radiotherapy in Patients with Prostate Cancer
Abstract
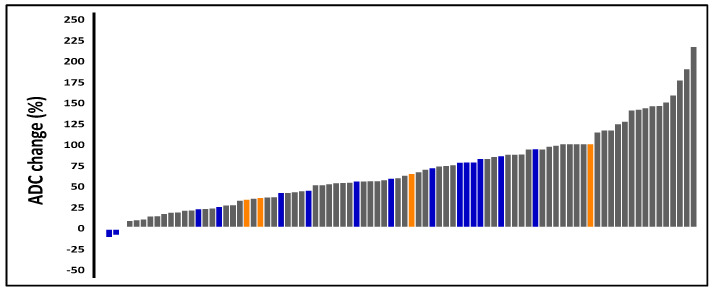
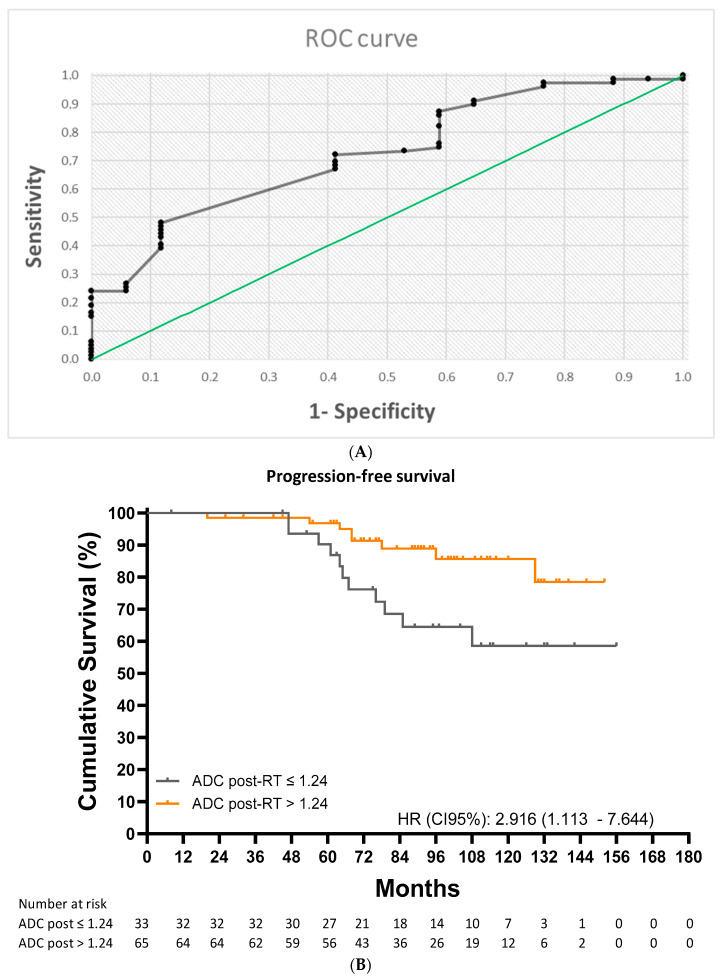
Background/Objectives: To analyze the predictive value of the apparent diffusion coefficient (ADC) in patients with prostate cancer (PCa) treated with radiotherapy (RT) and androgen deprivation therapy (ADT). Methods: Retrospective study of patients with high-risk, very high-risk, or unfavorable intermediate-risk PCa who received RT and ADT between 2008 and 2019 and underwent multiparametric magnetic resonance imaging mpMRI) at 6 months post-RT. Differences in ADC values were compared between patients with and without progression and/or local recurrence. Receiver operating characteristic (ROC) curves were used to obtain ADC cutoffs for predicting 10-year progression-free-survival (PFS) and local recurrence-free survival (LRFS). Results: We evaluated 98 patients (73 [74.5%] high-risk). Over a mean ± SD follow-up of 95.36 ± 30.54 months, 19 patients (19.4%) progressed; at 10 years, PFS was 75.6%, LRFS 93.8%, metastasis-free survival 85.5%, and overall survival 89.5%. Post-RT ADC was significantly lower in patients with local recurrence (1.09 ± 0.18 vs. 1.30 ± 0.20 × 10-3 mm2/s, p = 0.020) and progression (1.23 ± 0.20 vs. 1.30 ± 0.21 × 10-3 mm2/s, p = 0.004). ROC analysis identified a post-RT ADC cutoff of 1.11 × 10-3 mm2/s for local recurrence (area under curve [AUC] 0.843, sensitivity 89.4%, positive predictive value [PPV] 98.8%). The cutoff for progression was 1.24 × 10-3 mm2/s (AUC0.705, sensitivity 72.2%, PPV87.7%). Patients with a post-RT ADC value below and above 1.11 × 10-3 mm2/shad a 10-year LRFS of 66.8% and 97.7%, respectively (HR: 25.04 [2.58-242.92], p < 0.001). The corresponding rates for 10-year PFS were 58.6% and 85.6% in patients with post-RT ADC values below and above 1.24 × 10-3 mm2/s (HR: 2.916 [1.113-7.644], p = 0.015). In the multivariate analysis, a post-treatment ADC value ≤ 1.24 × 10-3 mm2/s was a significant prognostic factor for a lower PFS (HR: 3823 [1371-10,657], p = 0.010). Conclusions: This is the first study to show that post-RT ADC can be a predictive factor of local recurrence in PCa treated with RT and ADT. Moreover, this long-term study demonstrates its value as a predictive factor of progression in PCa treated with RT and ADT.
Keywords: androgen deprivation therapy; apparent diffusion coefficient; multiparametric magnetic resonance imaging; prostate cancer; radiotherapy.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures



References
-
- Neal D.E., Metcalfe C., Donovan J.L., Lane J.A., Davis M., Young G.J., Dutton S.J., Walsh E.I., Martin R.M., Peters T.J., et al. ProtecT Study Group. Ten-year Mortality, Disease Progression, and Treatment-related Side Effects in Men with Localised Prostate Cancer from the ProtecT Randomised Controlled Trial According to Treatment Received. Eur. Urol. 2020;77:320–330. doi: 10.1016/j.eururo.2019.10.030. Erratum in Eur. Urol. 2020, 78, e139–e143. - DOI - PubMed
-
- Duque-Santana V., Diaz-Gavela A., Recio M., Guerrero L.L., Peña M., Sanchez S., López-Campos F., Thuissard I.J., Andreu C., Sanz-Rosa D., et al. Jorge clinical study: 10-year outcomes of risk-adapted radiotherapy defined by multiparametric MRI for prostate cancer. World J. Urol. 2023;41:3829–3838. doi: 10.1007/s00345-023-04682-8. - DOI - PubMed
LinkOut - more resources
Full Text Sources
