

Clinical outcomes and molecular characteristics of lung-only and liver-only metastatic pancreatic cancer: results from a real-world evidence database
- PMID: 40079530
- PMCID: PMC11904785
- DOI: 10.1093/oncolo/oyaf007
Clinical outcomes and molecular characteristics of lung-only and liver-only metastatic pancreatic cancer: results from a real-world evidence database
Abstract
Background: Previous research demonstrates longer survival for patients with lung-only metastatic pancreatic adenocarcinoma (mPDAC) compared to liver-only mPDAC. The objective of this study is to understand the survival differences, impact of chemotherapy, and associated genomic features of mPDAC that is isolated to either the liver or lung.
Patients and methods: Longitudinal clinical outcomes and molecular sequencing data were retrospectively analyzed across 831 patients with PDAC across all stages whose tumors first metastasized to the liver or lung. Survival differences were evaluated using Cox regression. Mutational frequency differences were evaluated using Fisher's exact test.
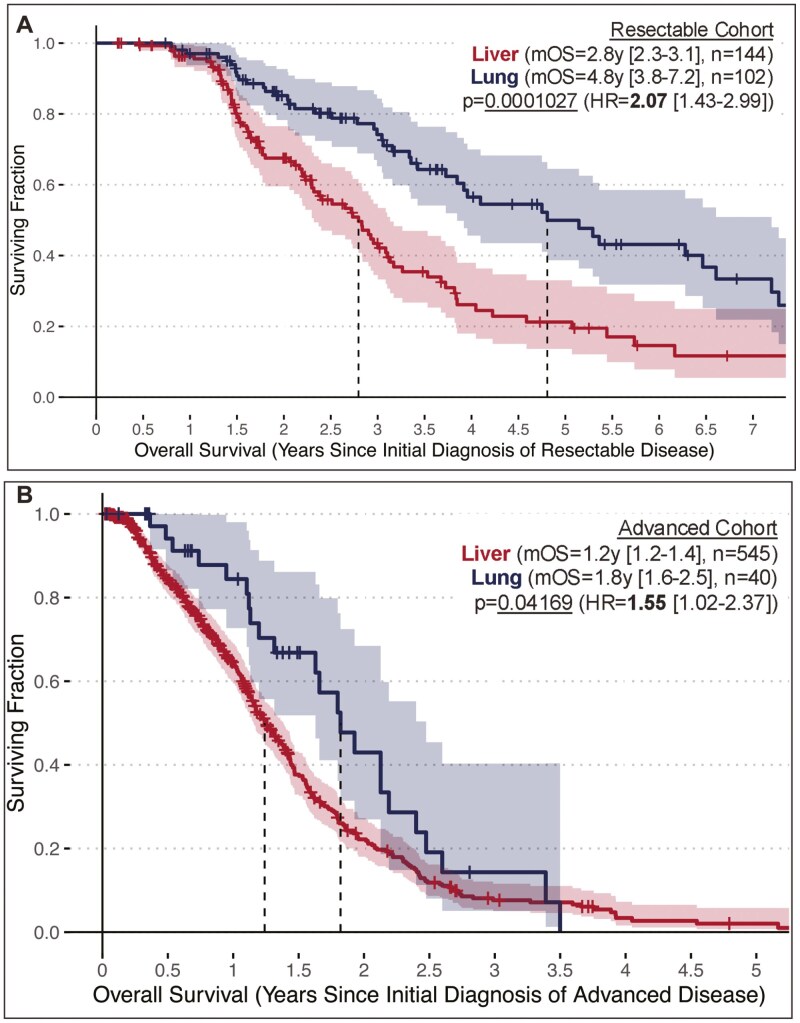
Results: Median overall survival (mOS) was shorter in patients with liver-only metastasis (1.3y [1.2-1.4], n = 689) compared to lung-only metastasis (2.1y [1.9-2.5], n = 142) (P = .000000588, HR = 2.00 [1.53-2.63]. Survival differences were observed regardless of choice of 1st-line standard-of-care therapy. For 5-fluorouracil-based therapies, mOS for liver-only mPDAC was 1.4y [1.3-1.6] (n = 211) compared to 2.1y [1.8-3.3] for lung-only mPDAC (n = 175) (P = .008113, HR = 1.75 [1.16-2.65]). For gemcitabine/nab-paclitaxel therapy, mOS for liver-only mPDAC was 1.2y [1.1-1.5] (n = 175) compared to 2.1y [1.6-3.4] for lung-only disease (n = 32) (P = .01863, HR = 1.84 [1.11-3.06]). PDAC tumors with liver-only metastases were modestly enriched (unadjustable P < .05) for: TP53 mutations, MYC amplifications, inactivating CDK2NA alterations, inactivating SMAD alterations, and SWI/SWF pathway mutations. PDAC tumors with lung-only metastases were enriched for: STK11 mutations, CCND1 amplifications, and GNAS alterations.
Conclusion: Patients with lung-only mPDAC demonstrate an improved prognosis relative to those with liver-only mPDAC. Responses to chemotherapy do not explain these differences. Organotropic metastatic tumor diversity is mirrored at the molecular level in PDAC.
Keywords: genetic profile; metastasis; pancreatic cancer; prognostic factors; treatment outcome.
© The Author(s) 2025. Published by Oxford University Press.
Conflict of interest statement
EB reports employment, inventor, and ownership interest at Perthera, Inc. RTS reports advisory board/consultation relationships with: AstraZeneca, Boehringer Ingelheim, Clovis, Genentech, Incyte, Merck, QED Therapeutics, Servier, Taiho, Zymeworks, Elevar Therapeutics, Ability Pharma, Duo Oncology, Hookipa Pharma, Natera, and Astellas. RTS also reports research funding from: Bayer, BMS, Bristol-Myers, Exelixis, IMV Inc., LOXO, Novocure, NUCANA, QED, Rafael Pharmaceuticals, Seagen, and Taiho. EP reports compensated consultation for: Perthera, Inc., Ignite Proteomics, Inc., and Ceres Nanosciences, Inc. MJP reports Ad Hoc Advisory roles for: AstraZeneca, Ideaya, Seattle Genetics, Merus, Merck, and Moderna. JG reports consultant or advisory roles for: Eisai, Exelixis, Janssen Biotech, Myovant/Pfizer, EMD Serono, Incyte, AVEO, Bayer, Seagan, Agenus, Taiho Pharmaceutical, and Caper Labs. All other authors have no known conflicts of interest to report currently.
Figures




References
-
- Siegel RL, Miller KD, Fuchs HE, Jemal A.. Cancer statistics, 2022. CA Cancer J Clin. 2022;72:7-33. https://doi.org/10.3322/caac.21708 - DOI - PubMed
-
- Rahib L, Wehner MR, Matrisian LM, Nead KT.. Estimated projection of US cancer incidence and death to 2040. JAMA Netw Open 2021;4:e214708. https://doi.org/10.1001/jamanetworkopen.2021.4708 - DOI - PMC - PubMed
-
- Park W, Chawla A, O’Reilly EM.. Pancreatic cancer: a review. JAMA. 2021;326:851-862. https://doi.org/10.1001/jama.2021.13027 - DOI - PMC - PubMed
-
- Sarnecka AK, Zagozda M, Durlik M.. An overview of genetic changes and risk of pancreatic ductal adenocarcinoma. J Cancer 2016;7:2045-2051. https://doi.org/10.7150/jca.15323 - DOI - PMC - PubMed
-
- Brar G, Blais EM, Joseph Bender R, et al.Multi-omic molecular comparison of primary versus metastatic pancreatic tumours. Br J Cancer. 2019;121:264-270. https://doi.org/10.1038/s41416-019-0507-5 - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
