

Epidemiology and transmission dynamics of multidrug-resistant organisms in nursing homes within the United States
- PMID: 40082431
- PMCID: PMC11906779
- DOI: 10.1038/s41467-025-57566-3
Epidemiology and transmission dynamics of multidrug-resistant organisms in nursing homes within the United States
Abstract
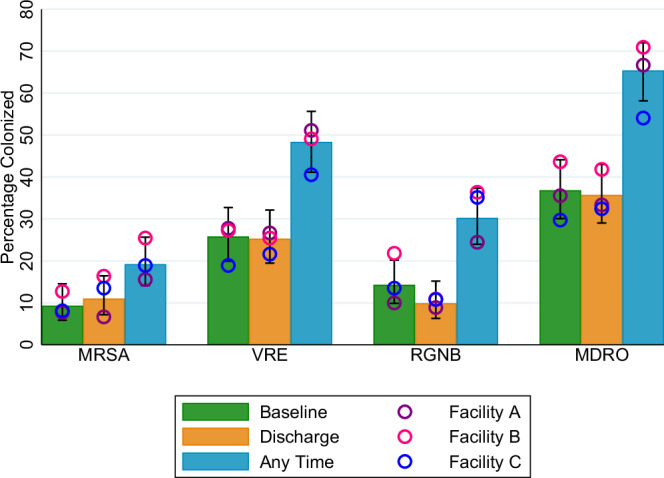
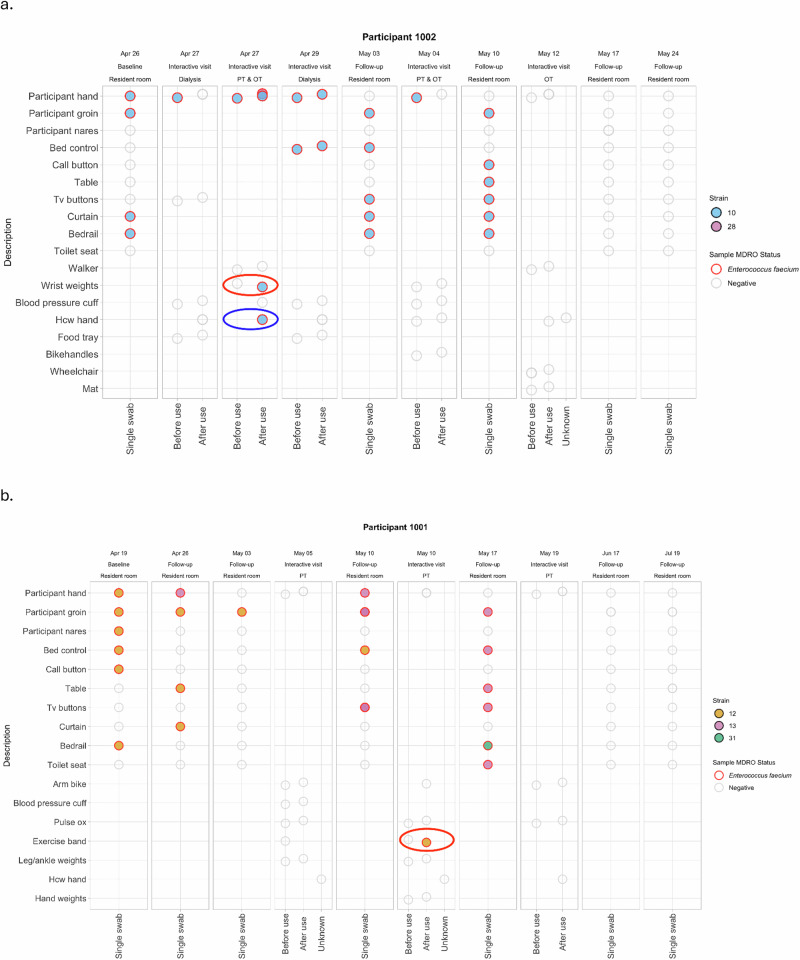
Nursing home (NH) residents in the United States routinely attend interactive visits for services such as therapy or dialysis, creating opportunities for pathogen transmission. A paucity of studies exist which delineate spread of pathogens beyond residents' in-room environment. In this prospective cohort study, we recruited 197 newly-admitted residents across three Veterans Affairs NHs to characterize multidrug-resistant organism (MDRO) prevalence, acquisition, and transmission. Participant hands, nares, groin, and seven environmental surfaces were swabbed during 758 regularly scheduled in-room visits; participant hands, healthcare personnel hands, and equipment were swabbed during 345 unscheduled interactive visits. We demonstrate that baseline MDRO colonization and new acquisition is common, and one in six interactive visits result in MDRO transmission. Whole genome sequencing on a subset of participants enabled us to identify sources of transmission where it was unknown using microbiologic methods alone. Our results illustrate MDRO transmission pathways and highlight the need for innovative, multidisciplinary interventions.
© 2025. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures



References
-
- White, H. K. Post-acute care: Current state and future directions. J. Am. Med Cir. Assoc.20, 392–395 (2019). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
