

Comparison of the analgesic efficacy of ultrasound-guided superficial serratus anterior plane block and intercostal nerve block for rib fractures: a randomized controlled trial
- PMID: 40082780
- PMCID: PMC11905462
- DOI: 10.1186/s12871-025-03000-6
Comparison of the analgesic efficacy of ultrasound-guided superficial serratus anterior plane block and intercostal nerve block for rib fractures: a randomized controlled trial
Abstract
Background: Various regional analgesic methods are frequently incorporated into multimodal analgesia strategies for managing rib fractures. This study aimed to compare the analgesic efficacy of ultrasound-guided superficial serratus anterior plane block (S-SAPB) and intercostal nerve block (ICNB) in patients with isolated rib fractures.
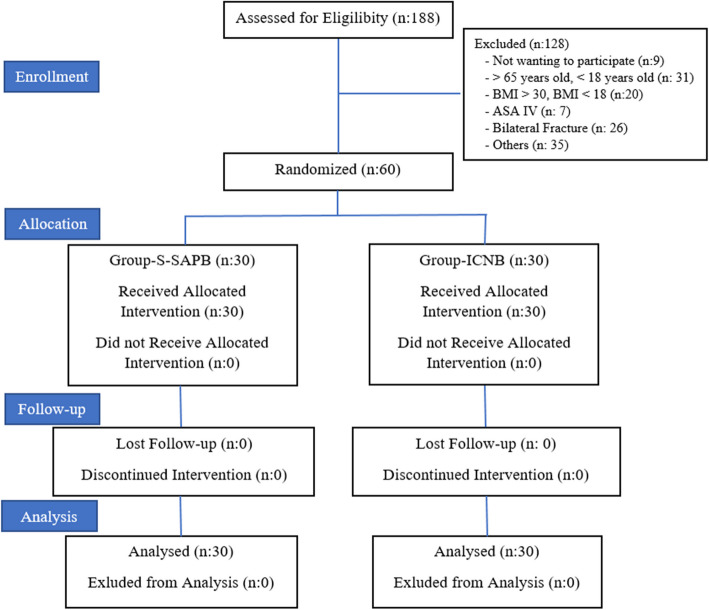
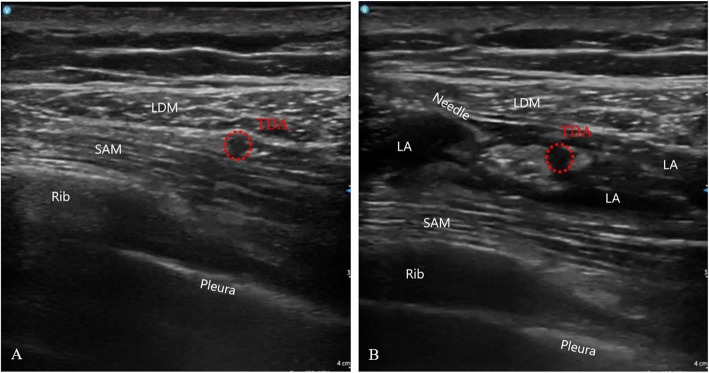
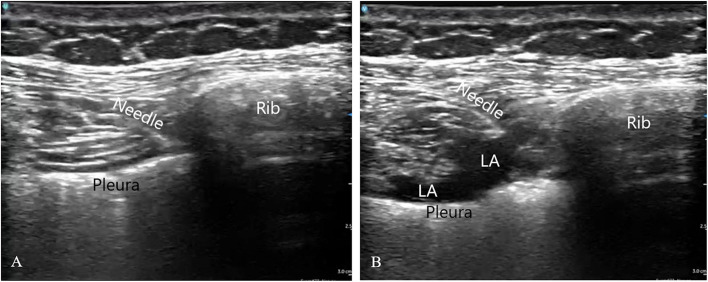
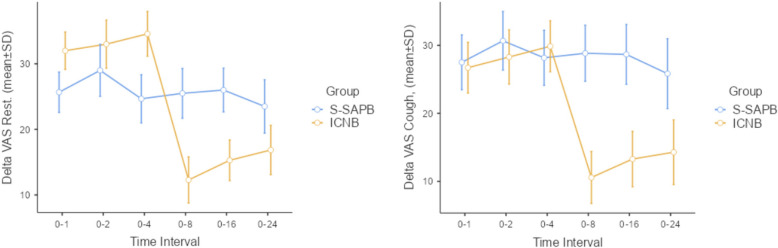
Methods: This randomized controlled trial included patients aged 18-65 years with unilateral isolated rib fractures (≤ 6 ribs) resulting from trauma. Patients underwent ultrasound-guided S-SAPB (20 ml 0.25% bupivacaine) or ICNB (3 ml 0.25% bupivacaine for each fractured rib). Pain levels were assessed using the Visual Analogue Scale (VAS) both prior to the procedure (Pre-Block, (T0)) and at specific time points following the intervention: 1st hour (T1), 2nd hour (T2), 4th hour (T4), 8th hour (T8), 16th hour (T16), and 24th hour (T24). The changes in observed values over time were expressed as delta (Δ).
Results: Both S-SAPB and ICNB provided effective analgesia. In the first 4 h, ICNB demonstrated a greater reduction in VAS scores, particularly in patients with 10th and 11th rib fractures. However, S-SAPB resulted in significantly longer-lasting analgesia, with greater pain relief after 8 h (T8-T24) compared to ICNB (p < 0.05). Patients in the S-SAPB group required no additional analgesia, whereas 43.3% of ICNB patients required supplemental tramadol (p < 0.001). Both techniques were well tolerated, with no reported complications.
Conclusions: S-SAPB provides prolonged analgesia and may be preferable for managing rib fracture pain beyond the initial 8 h. However, ICNB offers superior pain relief in the early postoperative period, especially for lower rib fractures (10th-11th ribs). A combined approach that includes both blocks may optimize pain control in patients with multiple rib fractures involving the 10th and 11th ribs.
Keywords: Intercostal nerve block; Pain; Plane blocks; Rib fracture; Serratus anterior plane block; Trauma.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Compliance with ethical standards: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration (as revised in 2013) and its later amendments or comparable ethical standards. Informed consent was obtained from all participants and was written in this study. Ethical approval: The study was conducted with a prospective and randomized design after obtaining approval from the Ankara Bilkent City Hospital Ethical Committee (E.Kurul-E1-21–2143, 01/12/2021) and written informed consent was obtained from all subjects participating in the trial. The trial was registered on www.clinicaltrials.gov ( https://clinicaltrials.gov/ ) under the identifier NCT05160155 on 15/12/2021. (principal investigator: Musa Zengin, MD). Informed consent: Patients were informed about the study, and their written consent was obtained. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures



References
-
- Ho AM, Karmakar MK, Critchley LA. Acute pain management of patients with multiple fractured ribs: a focus on regional techniques. Curr Opin Crit Care. 2011;17(4):323–7. - PubMed
-
- Shuaib W, Vijayasarathi A, Tiwana MH, Johnson JO, Maddu KK, Khosa F. The diagnostic utility of rib series in assessing rib fractures. Emerg Radiol. 2014;21(2):159–64. - PubMed
-
- Segers P, Van Schil P, Jorens P, Van Den Brande F. Thoracic trauma: an analysis of 187 patients. Acta Chir Belg. 2001;101(6):277–82. - PubMed
-
- Ziegler DW, Agarwal NN. The morbidity and mortality of rib fractures. J Trauma. 1994;37(6):975–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
