

Outcomes of ventricular tachycardia ablation facilitated by pre-procedural cardiac imaging-derived scar characterization: a prospective multi-centre international registry
- PMID: 40085771
- PMCID: PMC11983391
- DOI: 10.1093/europace/euaf051
Outcomes of ventricular tachycardia ablation facilitated by pre-procedural cardiac imaging-derived scar characterization: a prospective multi-centre international registry
Abstract
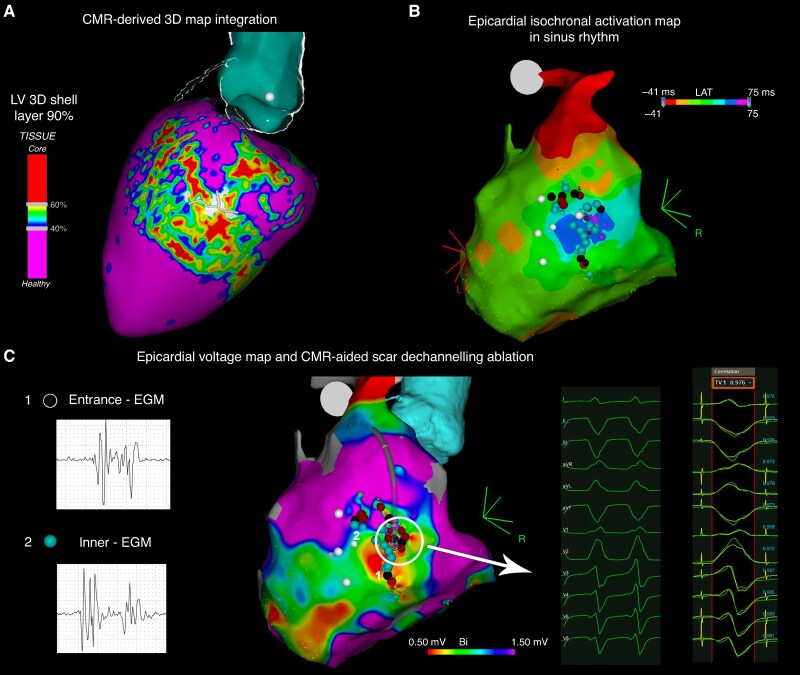
Aims: Pre-procedural imaging can facilitate scar-related ventricular tachycardia (VT) ablation, although only limited data have been reported. This prospective registry aimed to analyse procedural data and outcomes in a multi-centre setting of a pre-defined VT ablation strategy facilitated by the integration of pre-procedural imaging into the navigation system.
Methods and results: Consecutive patients referred for scar-related left-sided VT ablation were prospectively enrolled at five European tertiary hospitals. Pre-procedural cardiac magnetic resonance (CMR)-derived scar maps and/or multi-detector computed tomography (MDCT)-derived wall thinning maps of the left ventricle (LV) were obtained and integrated into the navigation system. An endocardial or endoepicardial approach was chosen based on the scar distribution at pre-procedural imaging. The decision of performing a detailed electro-anatomical map (EAM) of the LV (image-aided) or to using the pre-procedural imaging for guiding the ablation without obtaining an EAM (image-guided) was left to the physician's discretion. One hundred and seventy-one patients (71% with ischaemic cardiomyopathy) were included. Cardiac magnetic resonance was integrated in 159 (93%), MDCT in 113 (66%), and both in 101 (59%) procedures. Procedure-related complications occurred in 9 (5%) patients. At a mean follow-up of 18 ± 19 months, the overall survival and VT recurrence-free survival were 91 and 74.4%, respectively. There were no significant differences in long-term ablation outcomes based on the type of cardiomyopathy (P = 0.88) or the pre-procedural imaging modality employed (P = 0.33). An image-guided approach appears feasible, safe, and faster, with reduced procedure, radiofrequency, and fluoroscopy times, without compromising efficacy.
Conclusion: In a large multi-centre prospective cohort, VT ablation facilitated by pre-procedural imaging is associated with favourable long-term outcomes.
Keywords: Cardiac imaging; Cardiac magnetic resonance; Catheter ablation; Multi-detector computed tomography; Structural heart disease; Substrate ablation; Ventricular tachycardia.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: A.Ber. is stockholder of Galgo Medical. D.S.-I. and P.F.-O. are employees of Biosense Webster. P.F. received speaker fees from Boston Scientific and research grants from Abbott and Boston Scientific. All remaining authors have declared no conflicts of interest.
Figures







References
-
- Kuck KH, Schaumann A, Eckardt L, Willems S, Ventura R, Delacrétaz E et al. Catheter ablation of stable ventricular tachycardia before defibrillator implantation in patients with coronary heart disease (VTACH): a multicentre randomised controlled trial. Lancet 2010;375:31–40. - PubMed
-
- Arenal A, Avila P, Jimenez-Candil J, Tercedor L, Calvo D, Arribas F et al. Substrate ablation vs antiarrhythmic drug therapy for symptomatic ventricular tachycardia. J Am Coll Cardiol 2022;79:1441–53. - PubMed
-
- Kanagaratnam A, Virk SA, Pham T, Anderson RD, Turnbull S, Campbell T et al. Catheter ablation for ventricular tachycardia in ischaemic versus non-ischaemic cardiomyopathy: a systematic review and meta-analysis. Heart Lung Circ 2022;31:1064–74. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
