

Dynamic handgrip exercise for the detection of myocardial ischemia using fast Strain-ENCoded cardiovascular magnetic resonance
- PMID: 40086634
- PMCID: PMC12076776
- DOI: 10.1016/j.jocmr.2025.101879
Dynamic handgrip exercise for the detection of myocardial ischemia using fast Strain-ENCoded cardiovascular magnetic resonance
Abstract
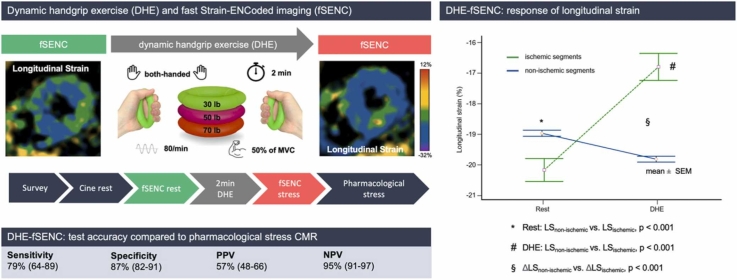
Background: Previous data suggest dynamic handgrip exercise (DHE) as a potential physiological, needle-free stressor feasible for cardiovascular magnetic resonance (CMR) examinations. DHE-fast Strain-ENCoded imaging (fSENC) is potentially cost-saving, ultra-fast and avoids pharmacological side effects thereby targeting the drawbacks of conventional pharmacological stress CMR.
Objectives: To assess the diagnostic accuracy of DHE-fSENC for detecting ischemia-related wall motion abnormalities in suspected obstructive coronary artery disease (CAD).
Methods: Patients with known or suspected obstructive CAD referred for CMR stress testing were prospectively enrolled. Diagnostic accuracy was assessed in comparison to pharmacological stress CMR and in a subgroup, compared to invasive coronary angiography (ICA). The CMR protocol was extended by both-handed DHE with 80 repetitions per minute over 2 min followed by fSENC short-axis acquisition before pharmacological stress testing. Stress-induced impairment of regional longitudinal strain was graded suspicious for obstructive CAD.
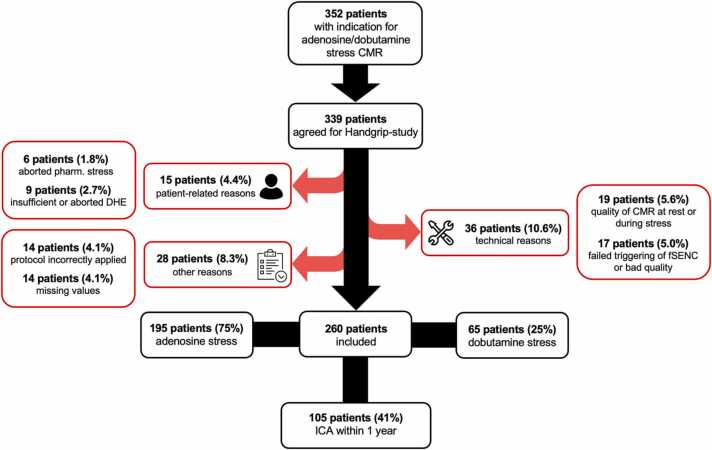
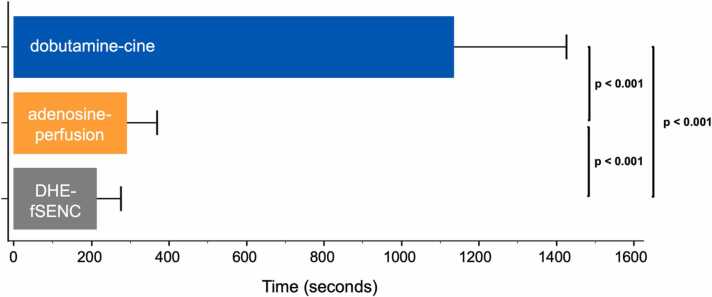
Results: Two-hundred sixty individuals with cardiovascular high-risk profile (64±13years, 75% male) were enrolled. DHE-fSENC provided a sensitivity of 79% (95% CI: 64-89) and specificity of 87% (95% CI 82-91) compared to pharmacological stress CMR. In a subgroup of 105 patients with recent ICA, high diagnostic accuracy was found for the detection of obstructive CAD (sensitivity 82% [95% CI: 67-92], specificity 89% [95% CI: 78-95]). Exam duration of DHE-fSENC was significantly reduced compared to conventional CMR stress protocols (DHE-fSENC 207±69 s vs. adenosine-perfusion 287±82 s vs. dobutamine-cine 1132±294 s, all p<0.001).
Conclusion: DHE-fSENC allows for a reliable and fast detection of obstructive CAD, thereby expanding the applicability of needle-free CMR stress testing.
Keywords: CMR; FSENC; Handgrip; Ischemia; Longitudinal strain.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Nael Osman reports a relationship with Myocardial Solutions Inc. that includes employment. Other authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures



References
-
- Nagel E., Greenwood J.P., McCann G.P., Bettencourt N., Shah A.M., Hussain S.T., et al. Magnetic resonance perfusion or fractional flow reserve in coronary disease. N Engl J Med. 2019;380(25):2418–2428. - PubMed
-
- Knuuti J., Ballo H., Juarez-Orozco L.E., Saraste A., Kolh P., Rutjes A.W.S., et al. The performance of non-invasive tests to rule-in and rule-out significant coronary artery stenosis in patients with stable angina: a meta-analysis focused on post-test disease probability. Eur Heart J. 2018;39(35):3322–3330. - PubMed
-
- Knuuti J., Wijns W., Saraste A., Capodanno D., Barbato E., Funck-Brentano C., et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41(3):407–477. - PubMed
-
- Korosoglou G., Elhmidi Y., Steen H., Schellberg D., Riedle N., Ahrens J., et al. Prognostic value of high-dose dobutamine stress magnetic resonance imaging in 1,493 consecutive patients: assessment of myocardial wall motion and perfusion. J Am Coll Cardiol. 2010;56(15):1225–1234. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
