

The Systemic Inflammatory Response Syndrome and Predictors of Infection and Mortality in 1068 Critically Ill Newborn Foals
- PMID: 40091577
- PMCID: PMC11911538
- DOI: 10.1111/jvim.70004
The Systemic Inflammatory Response Syndrome and Predictors of Infection and Mortality in 1068 Critically Ill Newborn Foals
Abstract
Background: Sepsis has been defined in humans as the concurrent proven or suspected presence of microbial infection and the systemic inflammatory response syndrome (SIRS). Sepsis is the leading cause of morbidity and mortality in neonatal foals. The clinical utility of using SIRS or its individual components to predict infection and mortality in critically ill foals is currently unknown.
Objectives: Assess the ability of history and signalment, clinical findings, laboratory results, and SIRS-related indices to predict infection and mortality in critically ill foals.
Animals: Retrospective, multi-center, cross-sectional study using a convenience sample of 1068 critically ill foals < 3 days of age admitted to 16 veterinary referral hospitals in 4 countries.
Methods: Data were retrieved from medical records. Infection was defined as the presence of bacteremia (positive blood culture) or clinical identification of an infected focus on admission. Univariate non-parametric and categorical methods, multivariate logistic regression, and classification tree methods were used for statistical analysis.
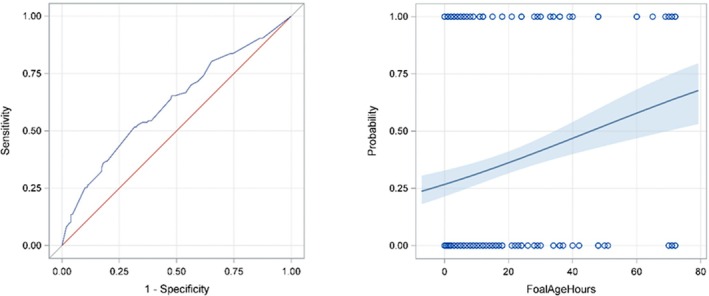
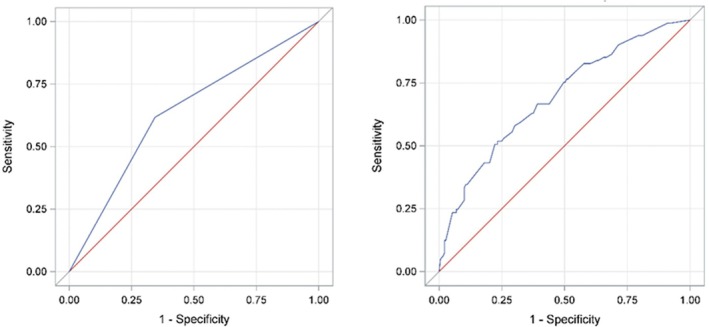
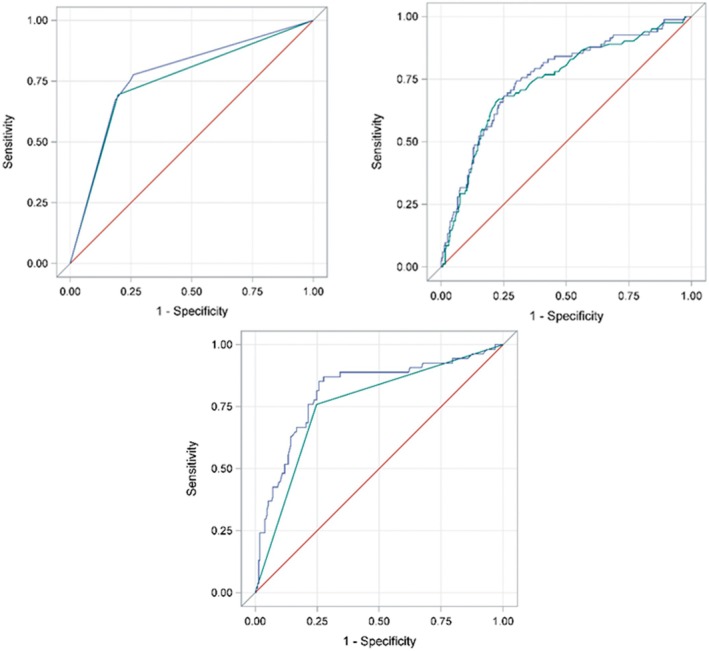
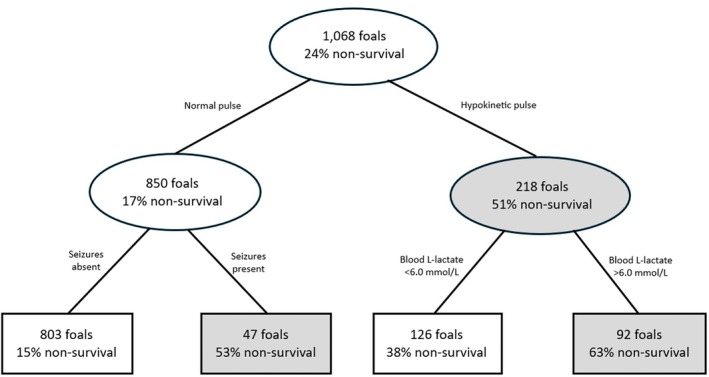
Results: Foal age at admission and presence of toxic neutrophils were independent predictors of infection, whereas SIRS-related indices were not predictive of infection. In-hospital mortality was 24%. Independent predictors for mortality were hypokinetic pulses, cold extremities, presence of seizures, blood L-lactate concentration > 6.0 mmol/L, and increased serum potassium and total bilirubin concentrations.
Conclusions and clinical importance: The presence of infection in critically ill newborn foals was not predicted by SIRS indices. Cardiovascular dysfunction was strongly associated with mortality, suggesting that maintaining adequate perfusion and pulse pressure should be important treatment goals.
Keywords: bacteremia; hyperlactatemia; sepsis; shock.
© 2025 The Author(s). Journal of Veterinary Internal Medicine published by Wiley Periodicals LLC on behalf of American College of Veterinary Internal Medicine.
Conflict of interest statement
Authors declare no off‐label use of antimicrobials.
The authors declare no conflicts of interest.
Figures
Similar articles
-
Arterial lactate concentration, hospital survival, sepsis and SIRS in critically ill neonatal foals.Equine Vet J. 2005 Jan;37(1):53-9. doi: 10.2746/0425164054406856. Equine Vet J. 2005. PMID: 15651735
-
Utility of cell-free DNA concentrations and illness severity scores to predict survival in critically ill neonatal foals.PLoS One. 2021 Apr 26;16(4):e0242635. doi: 10.1371/journal.pone.0242635. eCollection 2021. PLoS One. 2021. PMID: 33901192 Free PMC article.
-
Blood glucose concentrations in critically ill neonatal foals.J Vet Intern Med. 2008 Sep-Oct;22(5):1223-7. doi: 10.1111/j.1939-1676.2008.0174.x. Epub 2008 Aug 6. J Vet Intern Med. 2008. PMID: 18691362
-
Defining the Systemic Inflammatory Response Syndrome in Equine Neonates.Vet Clin North Am Equine Pract. 2015 Dec;31(3):463-81. doi: 10.1016/j.cveq.2015.08.001. Vet Clin North Am Equine Pract. 2015. PMID: 26612743 Review.
-
Prognostic Indicators for Survival and Athletic Outcome in Critically Ill Neonatal Foals.Vet Clin North Am Equine Pract. 2015 Dec;31(3):615-28. doi: 10.1016/j.cveq.2015.09.006. Vet Clin North Am Equine Pract. 2015. PMID: 26612751 Review.
Cited by
-
Hematologic Ratios in Donkeys: Reference Intervals and Response to Experimentally Induced Endotoxemia.Animals (Basel). 2025 Aug 4;15(15):2272. doi: 10.3390/ani15152272. Animals (Basel). 2025. PMID: 40805061 Free PMC article.
-
Assessment of Common Hematologic Parameters and Novel Hematologic Ratios for Predicting Piroplasmosis Infection in Horses.Animals (Basel). 2025 May 20;15(10):1485. doi: 10.3390/ani15101485. Animals (Basel). 2025. PMID: 40427362 Free PMC article.
-
An Overview of Donkey Neonatology.Animals (Basel). 2025 Jul 6;15(13):1986. doi: 10.3390/ani15131986. Animals (Basel). 2025. PMID: 40646885 Free PMC article. Review.
References
-
- Wong D., Wilkins P. A., and Landolt G., “Neonatal Infection,” Equine Neonatal Medicine (2024): 1126–1177.
-
- Fielding C. L. and Magdesian G. K., “Sepsis and Septic Shock in the Equine Neonate,” Veterinary Clinics of North America Equine Practice 31 (2015): 483–496. - PubMed
-
- Bone R. C., Balk R. A., Cerra F. B., et al., “Definitions for Sepsis and Organ Failure and Guidelines for the Use of Innovative Therapies in Sepsis the ACCP/SCCM Consensus Conference Committee,” Chest 101, no. 6 (1992): 1644–1655. - PubMed
