

Using Unsupervised Clustering to Characterize Phenotypes Among Older Kidney Transplant Recipients: A Cohort Study
- PMID: 40091888
- PMCID: PMC11909662
- DOI: 10.1177/20543581251322576
Using Unsupervised Clustering to Characterize Phenotypes Among Older Kidney Transplant Recipients: A Cohort Study
Abstract
Background: Older kidney transplant recipients have inferior outcomes compared to younger recipients, and this risk may be compounded by donor characteristics.
Objective: We applied an unsupervised machine learning clustering approach to group older recipients into similar phenotypes. We evaluated the association between each cluster and graft failure, and the impact of donor quality on outcomes.
Design: This is a nationally representative retrospective cohort study.
Setting and patients: Kidney transplant recipients aged ≥65 years identified from the Scientific Registry of Transplant Recipients (2000-2017).
Measurements and methods: We used unsupervised clustering to generate phenotypes using 16 recipient factors. Donor quality was evaluated using 2 approaches, including the Kidney Donor Risk Index (KDRI). All-cause graft failure was analyzed using multivariable Cox regression.
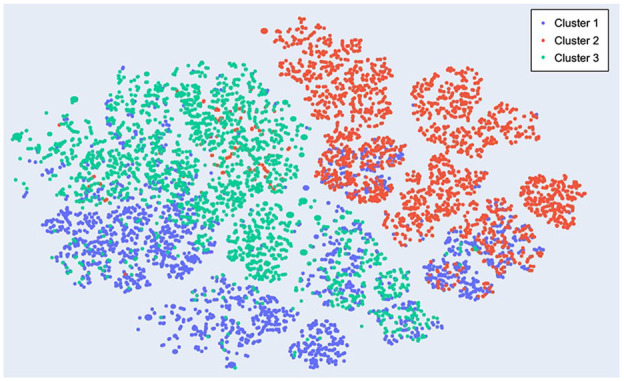
Results: Overall, 16 364 patients (mean age 69 years; 38% female) were separated into 3 clusters. Cluster 1 recipients were exclusively female; cluster 2 recipients were exclusively males without diabetes; and cluster 3 recipients were males with a higher burden of comorbidities. Compared to cluster 2, the risk of graft failure was higher for cluster 3 recipients (adjusted hazard ratio [aHR] = 1.25, 95% confidence interval [CI] = 1.19-1.32). Cluster 3 recipients of a lower quality (KDRI ≥1.45) kidney had the highest risk of graft failure (aHR = 1.74, 95% CI = 1.61-1.87) relative to cluster 2 recipients of a higher quality kidney.
Limitations: This study did not include an external validation cohort. The findings should be interpreted as exploratory and should not be used to inform individual risk prediction nor be applied to recipients <65 years of age.
Conclusions: In a national cohort of older kidney transplant recipients, unsupervised clustering generated 3 clinically distinct recipient phenotypes. These phenotypes may aid in complementing allocation decisions, providing prognostic information, and optimizing post-transplant care for older recipients.
Contexte: Les personnes plus âgées qui reçoivent une greffe de rein présentent des résultats de santé inférieurs à ceux des receveurs plus jeunes, et cette différence peut être aggravée par les caractéristiques du donneur.
Objectif: Nous avons appliqué une approche de regroupement par apprentissage automatique non supervisé pour regrouper des receveurs âgés avec des phénotypes similaires. Nous avons évalué l’association entre les caractéristiques des groupes formés et l’échec de la greffe, et examiné l’impact de la qualité du donneur sur les résultats.
Conception: Étude rétrospective d’une cohorte nationale représentative.
Cadre et sujets de l’étude: Les receveurs d’une greffe rénale âgés de 65 ans et plus identifiés à partir du Scientific Registry of Transplant Recipients (de 2000 à 2017).
Méthodologie et mesures: Nous avons utilisé le regroupement non supervisé pour générer des phénotypes à partir de 16 facteurs liés aux receveurs. La qualité des donneurs a été évaluée par deux approches, notamment le Kidney Donor Risk Index (KDRI). La défaillance du greffon toutes causes confondues a été analysée par régression de Cox multivariée.
Résultats: Au total, 16 364 patients (âge moyen: 69 ans; 38 % de femmes) ont été séparés en trois groupes. Le groupe 1 était constitué exclusivement de femmes; le groupe 2 était constitué exclusivement d’hommes non-diabétiques; et le groupe 3 était composé d’hommes présentant un fardeau plus important de comorbidités. Comparés aux sujets du groupe 2, les receveurs du groupe 3 présentaient un risque plus élevé d’échec du greffon (risque relatif corrigé [RRc]: 1,25; IC95: 1,19-1,32). Les sujets du groupe 3 qui avaient reçu un rein de moindre qualité (KDRI ≥ 1,45) présentaient le risque le plus élevé d’échec du greffon (RRc: 1,74; IC95: 1,61-1,87) lorsque comparés aux sujets du groupe 2 qui avaient reçu un rein de meilleure qualité.
Limites: Cette étude ne comportait pas de cohorte de validation externe. Les résultats doivent être interprétés comme étant exploratoires et ne devraient pas être utilisés pour éclairer la prévision du risque individuel ni être appliqués aux receveurs âgés de moins de 65 ans.
Conclusion: Dans une cohorte nationale constituée de personnes plus âgées recevant une greffe rénale, le regroupement non supervisé a généré trois phénotypes cliniquement distincts. Ces phénotypes pourraient aider à faciliter les décisions liées à l’attribution des organes, fournir des informations pronostiques et optimiser les soins post-transplantation pour les receveurs âgés.
Keywords: clustering; graft failure; kidney transplant; machine learning; older adults.
© The Author(s) 2025.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KKT has conducted advisory board groups and helped develop CME initiatives for Bayer, Otsuka, Vifor Pharmaceuticals, and Virtual Hallway, with no conflicts related to the current study. AJV has conducted advisory board groups for Paladin Labs Inc and Takeda Pharmaceuticals, with no conflicts related to the current study. All the other authors have no conflicts of interest to disclose.
Figures


Similar articles
-
Use of Machine Learning Consensus Clustering to Identify Distinct Subtypes of Black Kidney Transplant Recipients and Associated Outcomes.JAMA Surg. 2022 Jul 1;157(7):e221286. doi: 10.1001/jamasurg.2022.1286. Epub 2022 Jul 13. JAMA Surg. 2022. PMID: 35507356 Free PMC article.
-
Differences between Kidney Transplant Recipients from Deceased Donors with Diabetes Mellitus as Identified by Machine Learning Consensus Clustering.J Pers Med. 2023 Jul 3;13(7):1094. doi: 10.3390/jpm13071094. J Pers Med. 2023. PMID: 37511707 Free PMC article.
-
Clinical Phenotypes of Dual Kidney Transplant Recipients in the United States as Identified through Machine Learning Consensus Clustering.Medicina (Kaunas). 2022 Dec 12;58(12):1831. doi: 10.3390/medicina58121831. Medicina (Kaunas). 2022. PMID: 36557033 Free PMC article.
-
Distinct phenotypes of kidney transplant recipients aged 80 years or older in the USA by machine learning consensus clustering.BMJ Surg Interv Health Technol. 2023 Feb 20;5(1):e000137. doi: 10.1136/bmjsit-2022-000137. eCollection 2023. BMJ Surg Interv Health Technol. 2023. PMID: 36843871 Free PMC article.
-
Distinct Phenotypes of Kidney Transplant Recipients in the United States with Limited Functional Status as Identified through Machine Learning Consensus Clustering.J Pers Med. 2022 May 25;12(6):859. doi: 10.3390/jpm12060859. J Pers Med. 2022. PMID: 35743647 Free PMC article.
References
LinkOut - more resources
Full Text Sources
