

Wise Versus Vertical Mastopexy Pattern Skin-reducing Mastectomy With Immediate Breast Reconstruction: Systematic Review and Meta-analysis
- PMID: 40092505
- PMCID: PMC11908761
- DOI: 10.1097/GOX.0000000000006584
Wise Versus Vertical Mastopexy Pattern Skin-reducing Mastectomy With Immediate Breast Reconstruction: Systematic Review and Meta-analysis
Abstract
Background: This study compares postoperative outcomes of Wise and vertical mastopexy pattern skin-reducing/skin-sparing masctomy, hypothesizing that incision choice affects cosmetic outcomes and complication rates.
Methods: A systematic review and meta-analysis followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, searching PubMed, MEDLINE, Embase, Web of Science, and StarPlus Library. Included studies documented skin-sparing mastectomy using Wise or vertical mastopexy patterns with immediate reconstruction. The primary outcome is total mastectomy flap necrosis. The secondary outcomes are major/minor necrosis, infection, hematoma, seroma, and wound complications. Bayesian and frequentist generalized linear mixed models were used for the meta-analysis, including studies with 0 events.
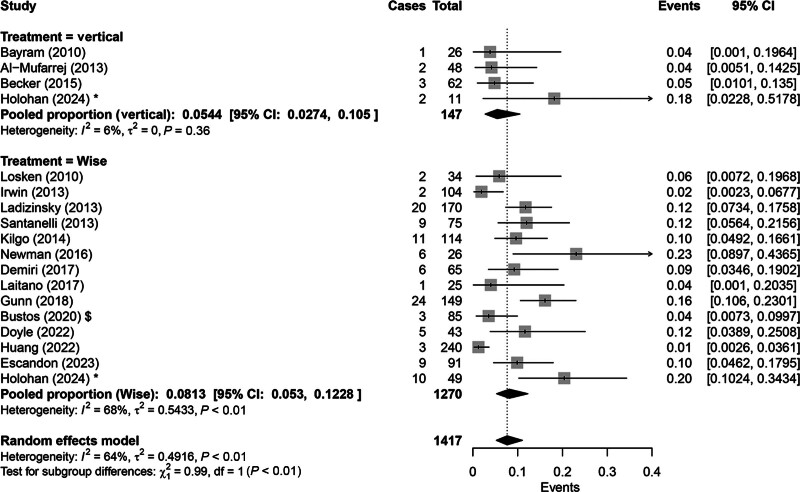
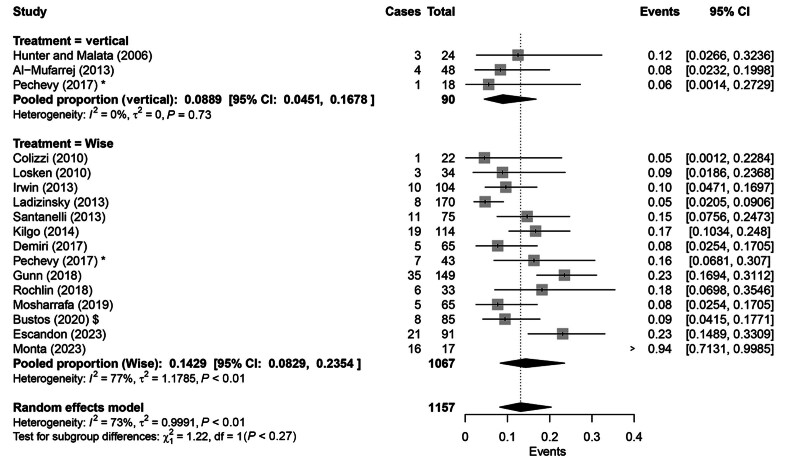
Results: Sixty-six studies were identified, with 39 included in the meta-analysis, comprising 1954 patients and 2311 breast reconstruction cases. The Wise group had a higher rate of mastectomy flap necrosis (14.2%; 95% confidence interval: 10%-20%; I² = 83%) compared with the vertical group (7.8%; 95% confidence interval: 5%-12%; I² = 0%) (P < 0.05). No significant differences were found in other domains. Subgroup analysis favored vertical mastopexy for wound-related complications (P = 0.04).
Conclusions: The Wise pattern shows significantly higher mastectomy flap necrosis than the vertical pattern. However, there were no significant differences in major necrosis, minor necrosis, infection, hematoma, or seroma. Future studies should focus on larger, high-quality randomized controlled trials to better understand the impact of incision techniques on postoperative outcomes.
Copyright © 2025 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of The American Society of Plastic Surgeons.
Conflict of interest statement
The authors have no financial interest to declare in relation to the content of this article. This study was funded by the University of Sheffield Open Access Fund. For the purpose of open access, the author has applied a Creative Commons Attribution (CC BY) license to any Author Accepted Manuscript version arising.
Figures









References
-
- Czajka ML, Pfeifer C. Breast Cancer Surgery. StatPearls Publishing; 2024. Available at http://www.ncbi.nlm.nih.gov/books/NBK553076/. Accessed July 17, 2024. - PubMed
-
- Audretsch WP, Rezai M, Kolotas C, et al. . Tumor-specific immediate reconstruction in breast cancer patients. Semin Plast Surg. 1998;11:71–100.
-
- Freeman BS. Subcutaneous mastectomy for benign breast lesions with immediate or delayed prosthetic replacement. Plast Reconstr Surg Transplant Bull. 1962;30:676–682. - PubMed
-
- Boneti CM, Yuen JM, Santiago CM, et al. . Oncologic safety of nipple skin-sparing or total skin-sparing mastectomies with immediate reconstruction. J Am Coll Surg. 2011;212:686–693. - PubMed
LinkOut - more resources
Full Text Sources