

Placental Location Site and Associated Intrapartum, Postpartum, and Neonatal Complications: A Comprehensive Review and Meta-Analysis
- PMID: 40095629
- PMCID: PMC11899809
- DOI: 10.3390/jcm14051649
Placental Location Site and Associated Intrapartum, Postpartum, and Neonatal Complications: A Comprehensive Review and Meta-Analysis
Abstract
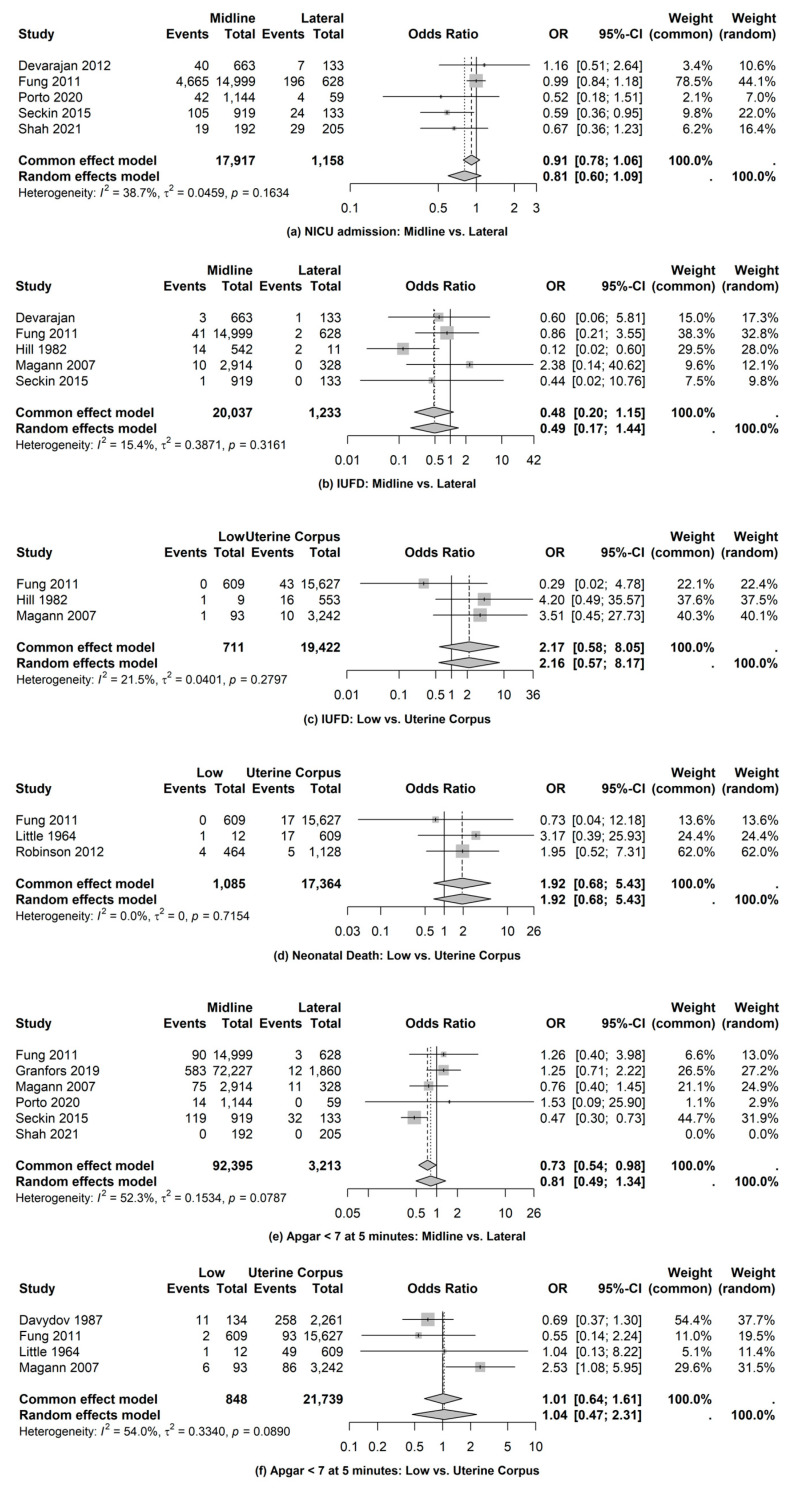
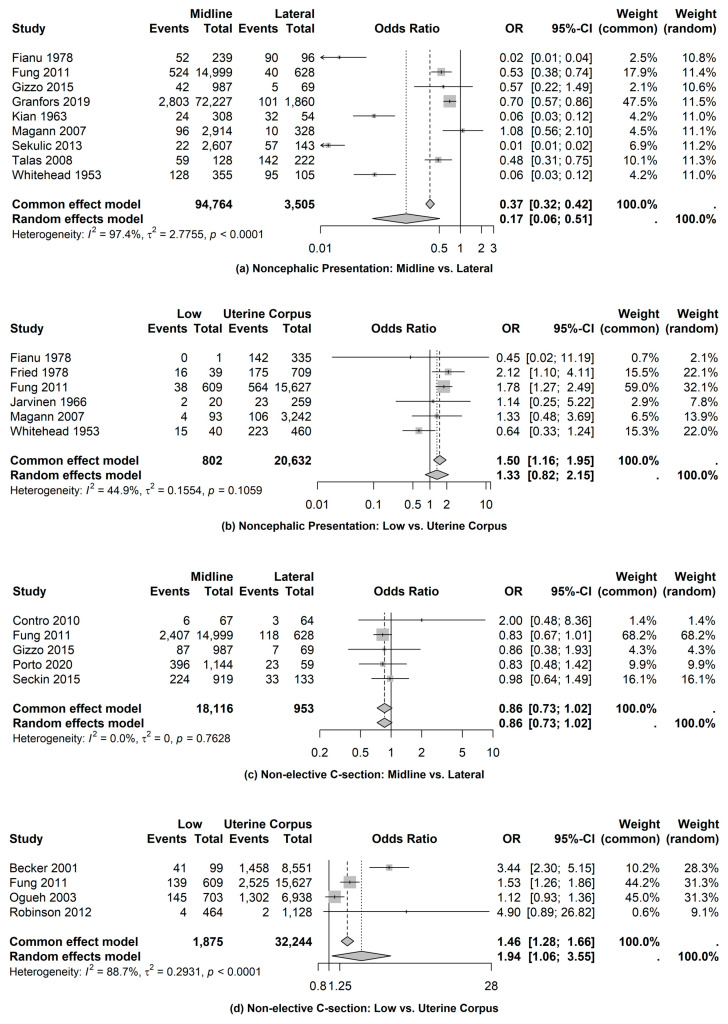
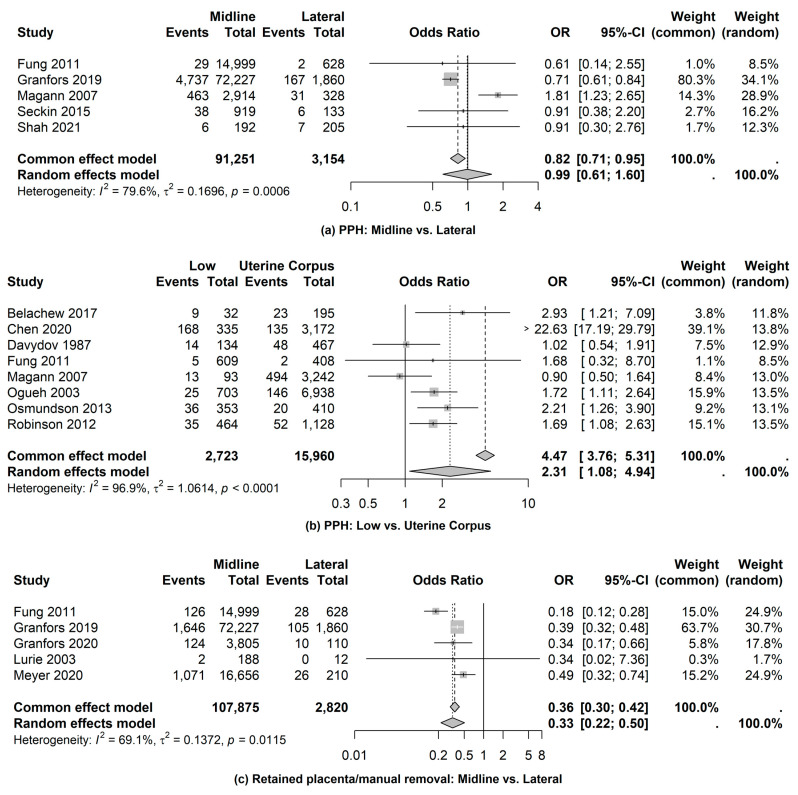
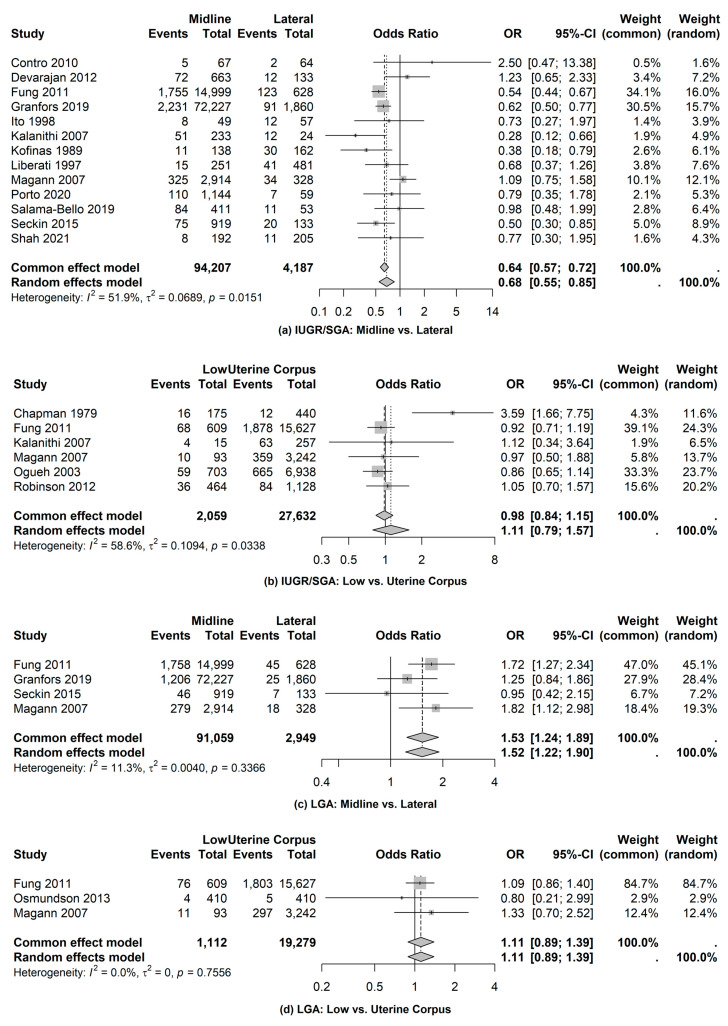
Background/Objectives: Adverse intrapartum, postpartum, and neonatal complications have been linked to placenta implantations sites. However, different reviews have led to contrasting conclusions about placental locations and pregnancy outcomes. We aim to determine if there is a relationship between the placental implantation site and intrapartum, postpartum, and neonatal outcomes. Methods: The Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines were followed during this review. The literature search used PubMed, CINAHL, and Embase. Years searched was not a study limitation. Only articles in English were included. Two authors reviewed the abstracts. Results: Of 40 articles identified as specific to intrapartum, postpartum, and/or neonatal complications (with some articles overlapping categories), 19 included intrapartum complications, 19 included postpartum complications, and 22 included neonatal complications. Pregnancies with a midline placenta (compared to a lateral placenta) had a greater likelihood of macrosomia/LGA infant (odds ratio (OR), 1.52 (95% CI: 1.22-1.90)) and lesser likelihood to have non-cephalic presentation (OR, 0.17 (95% CI: 0.06-0.51)), FGR/SGA infant (OR, 0.68 (CI: 0.55-0.85)), and retained placenta (OR, 0.33 (95% CI: 0.22-0.50)). Pregnancies with a low-lying placenta (compared to within uterine corpus) were more likely to have non-elective cesarean section (OR, 1.94 (95% CI: 1.06-3.55)) and postpartum hemorrhage (OR 1.49 (95% CI: 1.12-1.97)). Conclusions: Significant associations between placental location site and intrapartum complications (non-cephalic presentation, non-elective cesarean section), postpartum complications (postpartum hemorrhage, retained placenta), and neonatal complications (FGR/SGA, Macrosomia/LGA) were identified. There were no significant associations identified between the placental location site and several neonatal complications, including Apgar < 7 at 5 min, NICU admission, IUFD, and neonatal death.
Keywords: intrapartum complications; neonatal complications; placental location; postpartum complications.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Uterine artery Doppler in early labor and perinatal outcome in low-risk term pregnancy: prospective multicenter study.Ultrasound Obstet Gynecol. 2023 Aug;62(2):219-225. doi: 10.1002/uog.26199. Ultrasound Obstet Gynecol. 2023. PMID: 36905679
-
Emergency delivery in pregnancies at high probability of placenta accreta spectrum on prenatal imaging: a systematic review and meta-analysis.Am J Obstet Gynecol MFM. 2024 Oct;6(10):101432. doi: 10.1016/j.ajogmf.2024.101432. Epub 2024 Jul 26. Am J Obstet Gynecol MFM. 2024. PMID: 39069207
-
The relation between low-grade fever during prolonged rupture of membranes (>12 hours) at term and infectious outcomes: a retrospective cohort study.Am J Obstet Gynecol. 2024 Sep;231(3):361.e1-361.e10. doi: 10.1016/j.ajog.2024.05.054. Epub 2024 Jun 11. Am J Obstet Gynecol. 2024. PMID: 38871240
-
Second trimester placental location as a predictor of an adverse pregnancy outcome.J Perinatol. 2007 Jan;27(1):9-14. doi: 10.1038/sj.jp.7211621. Epub 2006 Nov 2. J Perinatol. 2007. PMID: 17080095
-
Placental location site and adverse antepartum pregnancy complications: a meta-analysis and review of the literature.Arch Gynecol Obstet. 2022 May;305(5):1265-1277. doi: 10.1007/s00404-021-06253-x. Epub 2021 Sep 29. Arch Gynecol Obstet. 2022. PMID: 34590170 Review.
References
-
- Stroup D.F., Berlin J.A., Morton S.C., Olkin I., Williamson G.D., Rennie D., Moher D., Becker B.J., Sipe T.A., Thacker S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283:2008–2012. doi: 10.1001/jama.283.15.2008. - DOI - PubMed
-
- Racher M.L., Morris M., Scott A.P., Ounpraseuth S.T., Hu Z., Whittington J.R., Quick C.M., Magann E.F. Placental location site and adverse antepartum pregnancy complications: A meta-analysis and review of the literature. Arch. Gynecol. Obstet. 2022;305:1265–1277. doi: 10.1007/s00404-021-06253-x. - DOI - PubMed
-
- Wells G., Shea B., O’Connell D., Peterson J., Welch V., Losos M., Tugwell P. The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. [(accessed on 22 January 2024)]. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
