

Multi-omic analysis of SDHB-deficient pheochromocytomas and paragangliomas identifies metastasis and treatment-related molecular profiles
- PMID: 40097403
- PMCID: PMC11914184
- DOI: 10.1038/s41467-025-57595-y
Multi-omic analysis of SDHB-deficient pheochromocytomas and paragangliomas identifies metastasis and treatment-related molecular profiles
Abstract
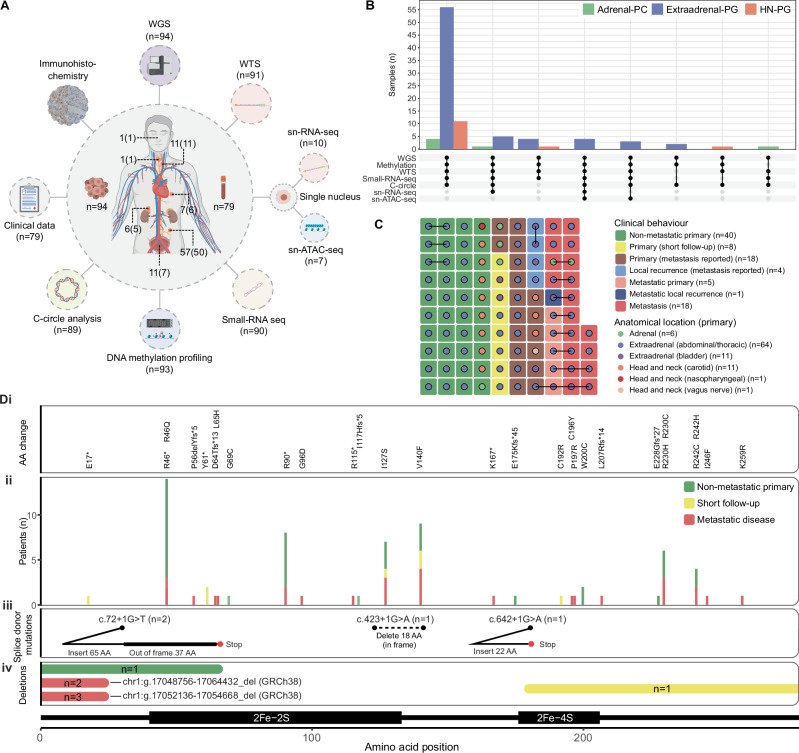
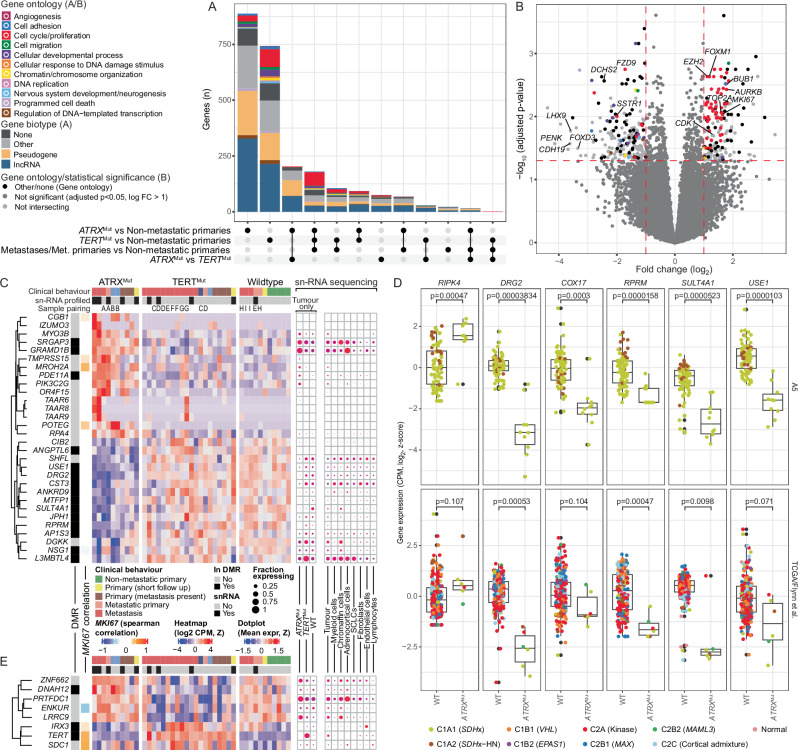
Hereditary SDHB-mutant pheochromocytomas (PC) and paragangliomas (PG) are rare tumours with a high propensity to metastasize although their clinical behaviour is unpredictable. To characterize the genomic landscape of these tumours and identify metastasis biomarkers, we perform multi-omic analysis on 94 tumours from 79 patients using seven molecular methods. Sympathetic (chromaffin cell) and parasympathetic (non-chromaffin cell) PCPG have distinct molecular profiles reflecting their cell-of-origin and biochemical profile. TERT and ATRX-alterations are associated with metastatic PCPG and these tumours have an increased mutation load, and distinct transcriptional and telomeric features. Most PCPG have quiet genomes with some rare co-operative driver events, including EPAS1/HIF-2α mutations. Two mechanisms of acquired resistance to DNA alkylating chemotherapies are identifiable; MGMT overexpression and mismatch repair-deficiency causing hypermutation. Our comprehensive multi-omic analysis of SDHB-mutant PCPG therefore identifies features of metastatic disease and treatment response, expanding our understanding of these rare neuroendocrine tumours.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures






Update of
-
Multi-omic analysis of SDHB-deficient pheochromocytomas and paragangliomas identifies metastasis and treatment-related molecular profiles.Res Sq [Preprint]. 2024 Jun 25:rs.3.rs-4410500. doi: 10.21203/rs.3.rs-4410500/v1. Res Sq. 2024. Update in: Nat Commun. 2025 Mar 17;16(1):2632. doi: 10.1038/s41467-025-57595-y. PMID: 38978571 Free PMC article. Updated. Preprint.
References
-
- Lenders, J. W. M. et al. Genetics, diagnosis, management and future directions of research of phaeochromocytoma and paraganglioma: a position statement and consensus of the Working Group on Endocrine Hypertension of the European Society of Hypertension. J. Hypertens.38, 1443–1456 (2020). - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
- TP828750/Victorian Cancer Agency (VCA)
- GM114102/U.S. Department of Health & Human Services | NIH | National Institute of General Medical Sciences (NIGMS)
- R01 GM114102/GM/NIGMS NIH HHS/United States
- APP1108032/Department of Health | National Health and Medical Research Council (NHMRC)
- CA264248/U.S. Department of Health & Human Services | NIH | NCI | Division of Cancer Epidemiology and Genetics, National Cancer Institute (National Cancer Institute Division of Cancer Epidemiology and Genetics)
LinkOut - more resources
Full Text Sources
Medical
Research Materials
