

A pilot study incorporating HER2-directed dendritic cells into neoadjuvant therapy of early stage HER2+ER- breast cancer
- PMID: 40097486
- PMCID: PMC11914126
- DOI: 10.1038/s41523-025-00742-x
A pilot study incorporating HER2-directed dendritic cells into neoadjuvant therapy of early stage HER2+ER- breast cancer
Abstract
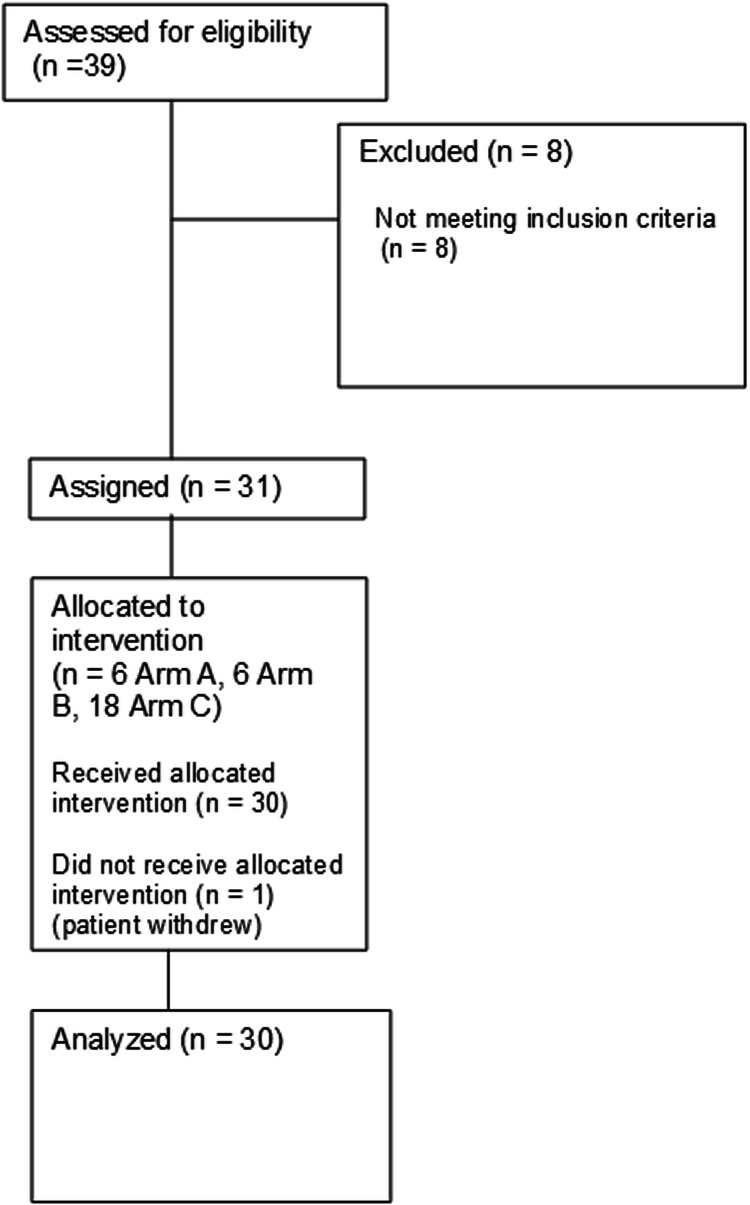
Type 1 dendritic cell vaccines targeting HER2 (HER2-DC1) reinvigorates antitumor immunity which correlates with neoadjuvant therapy response. A pilot trial (clinicaltrials.gov,NCT03387553,1/2/2018) using HER2-DC1 pre-neoadjuvant therapy evaluated feasibility/safety and pathologic response rates/immunogenicity. Stage II-III ER-HER2+ breast cancer patients prescribed neoadjuvant docetaxel/carboplatin/trastuzumab/pertuzumab (TCHP) were enrolled. HER2-DC1 (2×107 cells/vaccine) was given for 3 weeks prior to chemotherapy intranodal (IN) 1x/week (Arm A), IN 2x/week (Arm B), and 2x/week alternating intratumoral (IT) and IN (Arm C). HER2 ELISPOT counts (EHC) and immunofluorescence analysis of biopsies were performed. Six patients enrolled in Arms A and B, 18 patients in Arm C. Neoadjuvant HER2-DC1 demonstrated no unexpected safety signals. Pathologic complete response rates (pCR) across arms A, B, C were 42.8%, 66.6%, and 72.7%. Intranodal HER2-DC1 increased EHC, but IT + IN HER2-DC1 reduced EHC, possibly due to increased T cell tumor trafficking. Immunofluorescence showed increased T cell infiltration following IT + IN injections. Additional IT HER2-DC1 investigation is warranted.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: HS has consulted for: Eli Lilly, Astrazeneca, Novartis, PUMA, Pfizer, Sermonix. BN has research support from Hologic. RC has consulted for: Pfizer, Gilead, Daiichi Sankyo and Astra Zeneca Speaker’s Bureau for: Pfizer, Daiichi Sankyo, and Astra Zeneca Honoraria from: Pfizer, Athenex Oncology, Daiichi Sankyo and Astra Zeneca. HH received institutional research funding from: Arvinas, Abbvie, Pfizer, Zymeworks, Quantum Leap Health, Senwha, Mersana, Gilead Advisory Board: Paradigm, Pfizer. BC has intellectual property rights/licensure for DC1 vaccine from Immunorestoration. The remaining authors have not declared relevant COI.
Figures




References
Associated data
Grants and funding
- W81XWH-16-1-0385/United States Department of Defense | United States Army | Army Medical Command | Congressionally Directed Medical Research Programs (CDMRP)
- W81XWH-16-1-0385/United States Department of Defense | United States Army | Army Medical Command | Congressionally Directed Medical Research Programs (CDMRP)
- W81XWH-16-1-0385/United States Department of Defense | United States Army | Army Medical Command | Congressionally Directed Medical Research Programs (CDMRP)
- W81XWH-16-1-0385/United States Department of Defense | United States Army | Army Medical Command | Congressionally Directed Medical Research Programs (CDMRP)
- W81XWH-16-1-0385/United States Department of Defense | United States Army | Army Medical Command | Congressionally Directed Medical Research Programs (CDMRP)
- W81XWH-16-1-0385/United States Department of Defense | United States Army | Army Medical Command | Congressionally Directed Medical Research Programs (CDMRP)
- W81XWH-16-1-0385/United States Department of Defense | United States Army | Army Medical Command | Congressionally Directed Medical Research Programs (CDMRP)
- W81XWH-16-1-0385/United States Department of Defense | United States Army | Army Medical Command | Congressionally Directed Medical Research Programs (CDMRP)
- W81XWH-16-1-0385/United States Department of Defense | United States Army | Army Medical Command | Congressionally Directed Medical Research Programs (CDMRP)
- W81XWH-16-1-0385/United States Department of Defense | United States Army | Army Medical Command | Congressionally Directed Medical Research Programs (CDMRP)
- W81XWH-16-1-0385/United States Department of Defense | United States Army | Army Medical Command | Congressionally Directed Medical Research Programs (CDMRP)
- W81XWH-16-1-0385/United States Department of Defense | United States Army | Army Medical Command | Congressionally Directed Medical Research Programs (CDMRP)
- W81XWH-16-1-0385/United States Department of Defense | United States Army | Army Medical Command | Congressionally Directed Medical Research Programs (CDMRP)
- W81XWH-16-1-0385/United States Department of Defense | United States Army | Army Medical Command | Congressionally Directed Medical Research Programs (CDMRP)
- W81XWH-16-1-0385/United States Department of Defense | United States Army | Army Medical Command | Congressionally Directed Medical Research Programs (CDMRP)
- W81XWH-16-1-0385/United States Department of Defense | United States Army | Army Medical Command | Congressionally Directed Medical Research Programs (CDMRP)
- W81XWH-16-1-0385/United States Department of Defense | United States Army | Army Medical Command | Congressionally Directed Medical Research Programs (CDMRP)
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
