

Impact of prepared vascular access on mortality and medical expenses in elderly and non-elderly Japanese patients with chronic kidney disease stage G5: a retrospective cohort study
- PMID: 40100518
- PMCID: PMC12331761
- DOI: 10.1007/s10157-025-02654-3
Impact of prepared vascular access on mortality and medical expenses in elderly and non-elderly Japanese patients with chronic kidney disease stage G5: a retrospective cohort study
Abstract
Background: Patients with chronic kidney disease (CKD) stage 5 (CKDG5) have greater dialysis requirements that increase the risk of cardiovascular disease and mortality. The elevated costs associated with CKDG5 are a serious concern. The impact of prepared vascular access (VA) through planned VA creation on mortality and medical expenses remains unclear in Japanese patients with CKDG5.
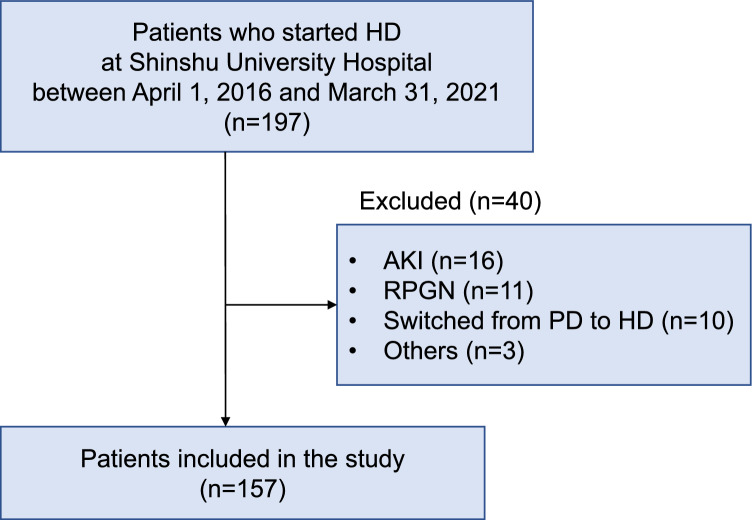
Methods: We conducted a retrospective cohort study including 157 patients with CKD who started hemodialysis (HD) at Shinshu University Hospital from April 2016 to March 2021 and assessed the relationship between the presence of a prepared VA and mortality and hospitalization expenses in elderly and non-elderly patients with CKDG5.
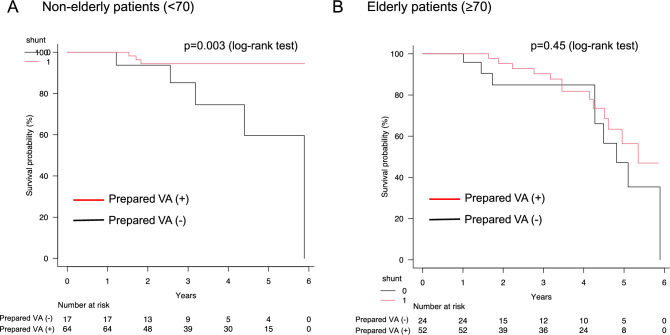
Results: The presence of a prepared VA was associated with lower mortality in non-elderly patients but not in elderly patients. Medical expenses, emergency HD, and hospitalization duration were significantly lower in patients with a prepared VA in both age groups. The contribution of a prepared VA to mortality and medical expenses remained consistent after adjusting for sex, performance status, comorbidities, and nutritional status.
Conclusion: A prepared VA showed several benefits, including lower mortality rates and hospitalization costs; shorter hospital stays; and higher home discharge rates. Planned VA creation was significantly associated with lower hospitalization expenses, irrespective of age.
Keywords: Elderly patients; Hemodialysis; Hospitalization expenses; Mortality; Vascular access.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflicts of interest: The authors have declared that no conflict of interest exists.
Figures
Similar articles
-
Early referral strategies for management of people with markers of renal disease: a systematic review of the evidence of clinical effectiveness, cost-effectiveness and economic analysis.Health Technol Assess. 2010 Apr;14(21):1-184. doi: 10.3310/hta14210. Health Technol Assess. 2010. PMID: 20441712
-
Hemodialysis vascular access in the elderly: Promising results from a tertiary center.Nefrologia (Engl Ed). 2025 Mar;45(3):228-237. doi: 10.1016/j.nefroe.2025.02.011. Nefrologia (Engl Ed). 2025. PMID: 40082052
-
Home versus in-centre haemodialysis for people with kidney failure.Cochrane Database Syst Rev. 2024 Apr 8;4(4):CD009535. doi: 10.1002/14651858.CD009535.pub3. Cochrane Database Syst Rev. 2024. PMID: 38588450 Free PMC article.
-
Multiple-frequency bioimpedance devices for fluid management in people with chronic kidney disease receiving dialysis: a systematic review and economic evaluation.Health Technol Assess. 2018 Jan;22(1):1-138. doi: 10.3310/hta22010. Health Technol Assess. 2018. PMID: 29298736 Free PMC article.
-
Blood pressure targets for hypertension in people with chronic renal disease.Cochrane Database Syst Rev. 2024 Oct 15;10(10):CD008564. doi: 10.1002/14651858.CD008564.pub3. Cochrane Database Syst Rev. 2024. PMID: 39403990
References
-
- Keith DS, Nichols GA, Gullion CM, Brown JB, Smith DH. Longitudinal follow-up and outcomes among a population with chronic kidney disease in a large managed care organization. Arch Intern Med. 2004;164:659–63. - PubMed
-
- Nakamura K, Okamura T, Hayakawa T, et al. Chronic kidney disease is a risk factor for cardiovascular death in a community-based population in Japan NIPPON DATA. Circ J. 2006;70(90):954–9. - PubMed
-
- Nakayama M, Sato T, Miyazaki M, et al. Increased risk of cardiovascular events and mortality among non-diabetic chronic kidney disease patients with hypertensive nephropathy: the Gonryo study. Hypertens Res. 2011;34:1106–10. - PubMed
-
- Ortega T, Ortega F, Diaz-Corte C, Rebollo P, Ma Baltar J, Alvarez-Grande J. The timely construction of arteriovenous fistulae: a key to reducing morbidity and mortality and to improving cost management. Nephrol Dial Transplant. 2005;20:598–603. - PubMed
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
