

Comprehensive immunophenotyping of gastric adenocarcinoma identifies an inflamed class of tumors amenable to immunotherapies
- PMID: 40102027
- PMCID: PMC11927434
- DOI: 10.1136/jitc-2024-010024
Comprehensive immunophenotyping of gastric adenocarcinoma identifies an inflamed class of tumors amenable to immunotherapies
Abstract
Background: Gastric adenocarcinoma (GAC) imposes a considerable global health burden. Molecular profiling of GAC from the tumor microenvironment perspective through a multi-omics approach is eagerly awaited in order to allow a more precise application of novel therapies in the near future.
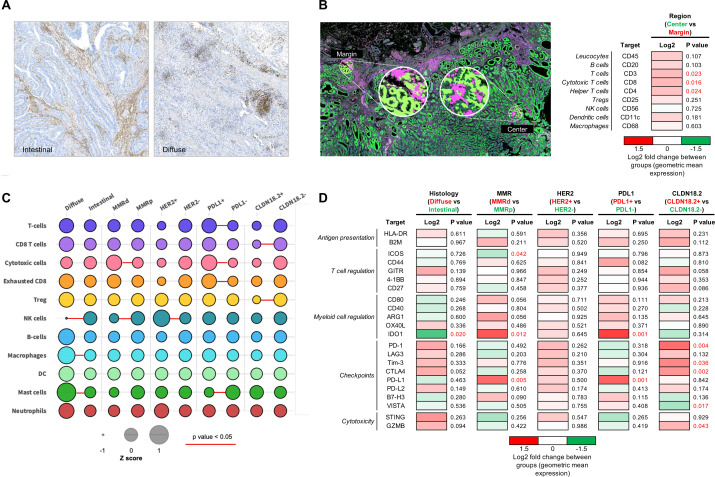
Methods: To better understand the tumor-immune interface of GAC, we identified an internal cohort of 82 patients that allowed an integrative molecular analysis including mutational profiling by whole-exome sequencing, RNA gene expression of 770 genes associated with immune response, and multiplex protein expression at spatial resolution of 34 immuno-oncology targets at different compartments (tumorous cells and immune cells). Molecular findings were validated in 595 GAC from the TCGA and ACRG external cohorts with available multiomics data. Prediction of response to immunotherapies of the discovered immunophenotypes was assessed in 1039 patients with cancer from external cohorts with available transcriptome data.
Results: Unsupervised clustering by gene expression identified a subgroup of GAC that includes 52% of the tumors, the so-called Inflamed class, characterized by high tumor immunogenicity and cytotoxicity, particularly in the tumor center at protein level, with enrichment of PIK3CA and ARID1A mutations and increased presence of exhausted CD8+ T cells as well as co-inhibitory receptors such as PD1, CTLA4, LAG3, and TIGIT. The remaining 48% of tumors were called non-inflamed based on the observed exclusion of T cell infiltration, with an overexpression of VEGFA and higher presence of TP53 mutations, resulting in a worse clinical outcome. A 10-gene RNA signature was developed for the identification of tumors belonging to these classes, demonstrating in evaluated datasets comparable clinical utility in predicting response to current immunotherapies when tested against other published gene signatures.
Conclusions: Comprehensive immunophenotyping of GAC identifies an inflamed class of tumors that complements previously proposed tumor-based molecular clusters. Such findings may provide the rationale for exploring novel immunotherapeutic approaches for biomarker-enriched populations in order to improve GAC patient's survival.
Keywords: Biomarker; Gastric Cancer; Immunotherapy.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: JVR has received lecture fees from MSD and travel and education funding from MSD, Astrazeneca, Ipsen, Advanz pharma and AAA. RM has received consulting and lecture fees from Servier, Roche and Bristol Myers Squibb and travel and education funding from MSD, Eli Lilly, Bayer, Roche, Astrazeneca.
Figures




References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous