

Combined apophyseal and epiphyseal fixation of Ogden type IIIA/IV tibial tubercle avulsion fractures provides favorable stability compared to isolated apophyseal screw fixation - a biomechanical study
- PMID: 40102219
- PMCID: PMC11920350
- DOI: 10.1007/s00068-025-02814-w
Combined apophyseal and epiphyseal fixation of Ogden type IIIA/IV tibial tubercle avulsion fractures provides favorable stability compared to isolated apophyseal screw fixation - a biomechanical study
Abstract
Purpose: Current literature lacks recommendations regarding proper fixation of tibial tubercle avulsion fractures involving the proximal tibial epiphysis (Ogden fractures). Therefore, the aim of this study was to compare isolated apophyseal screw fixation and additional fixation techniques in Ogden fractures.
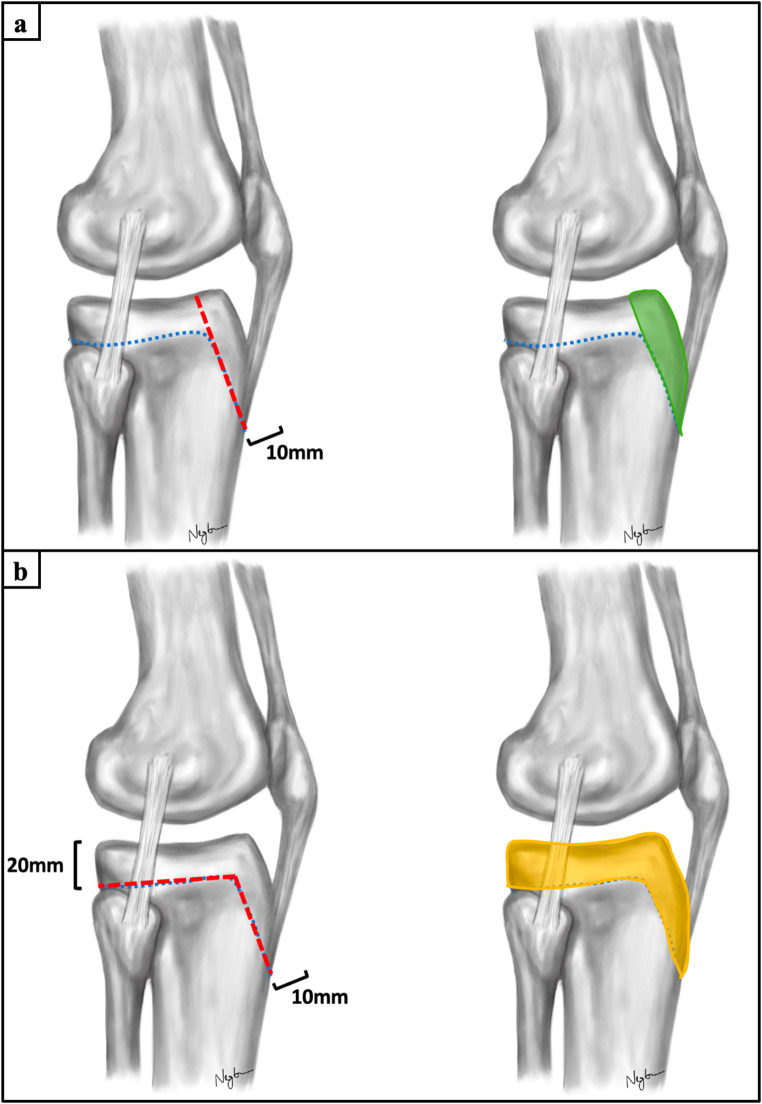
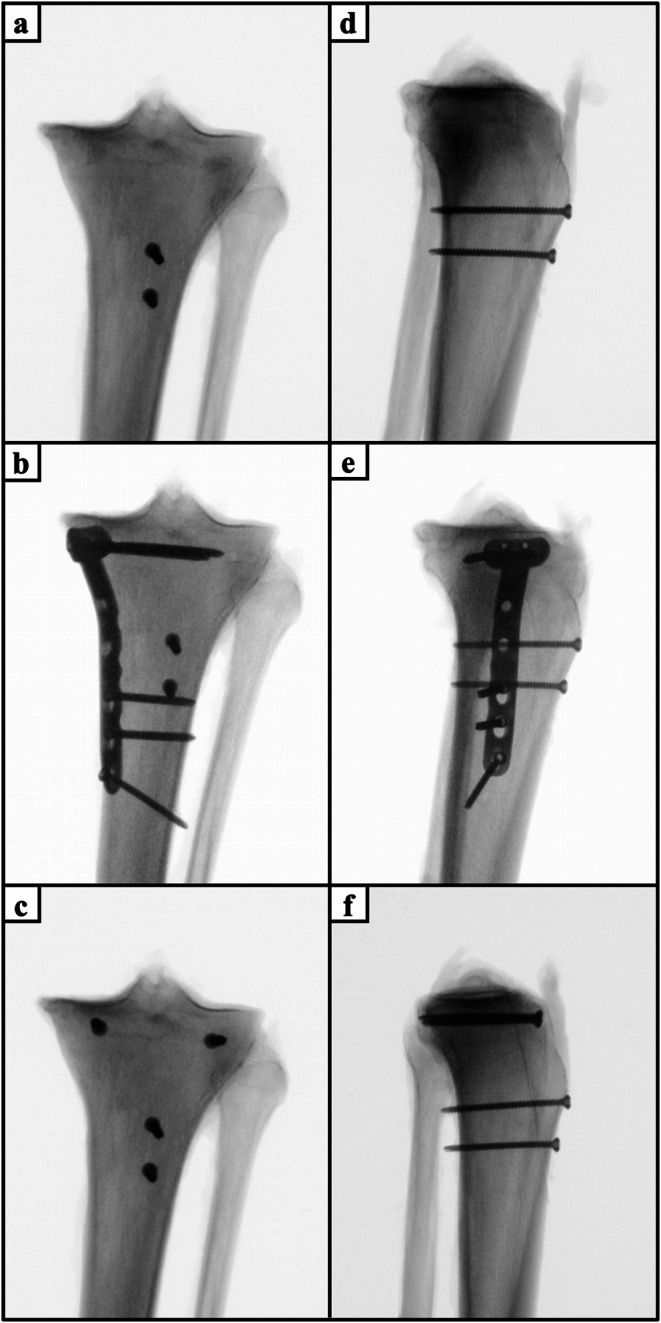
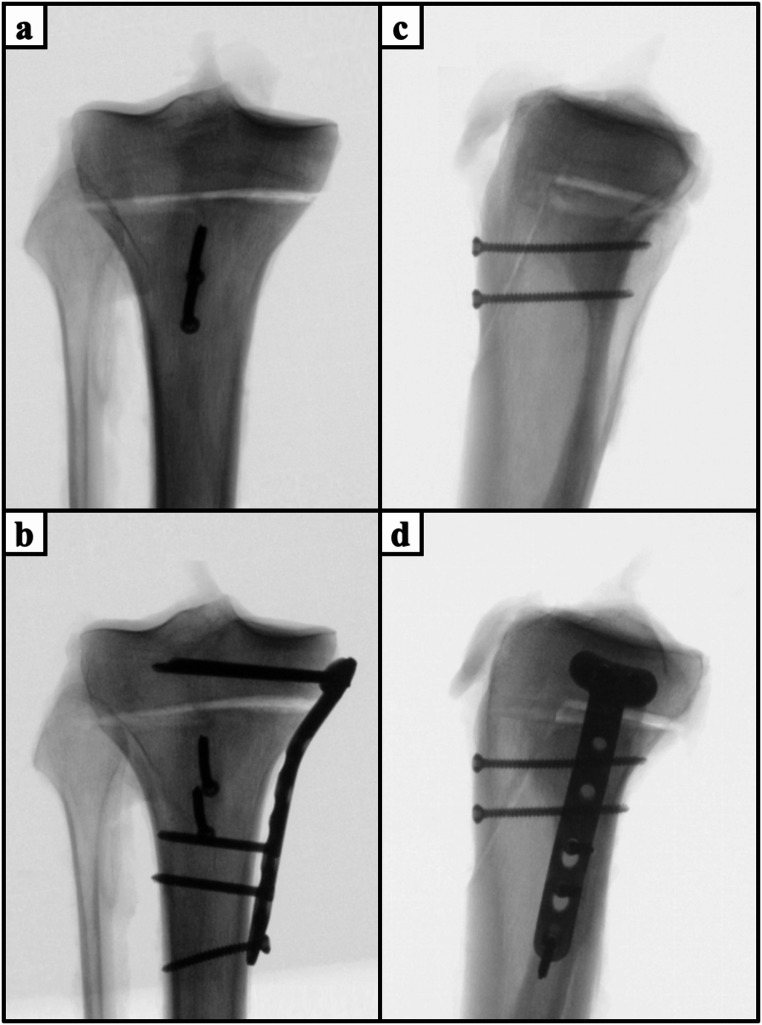
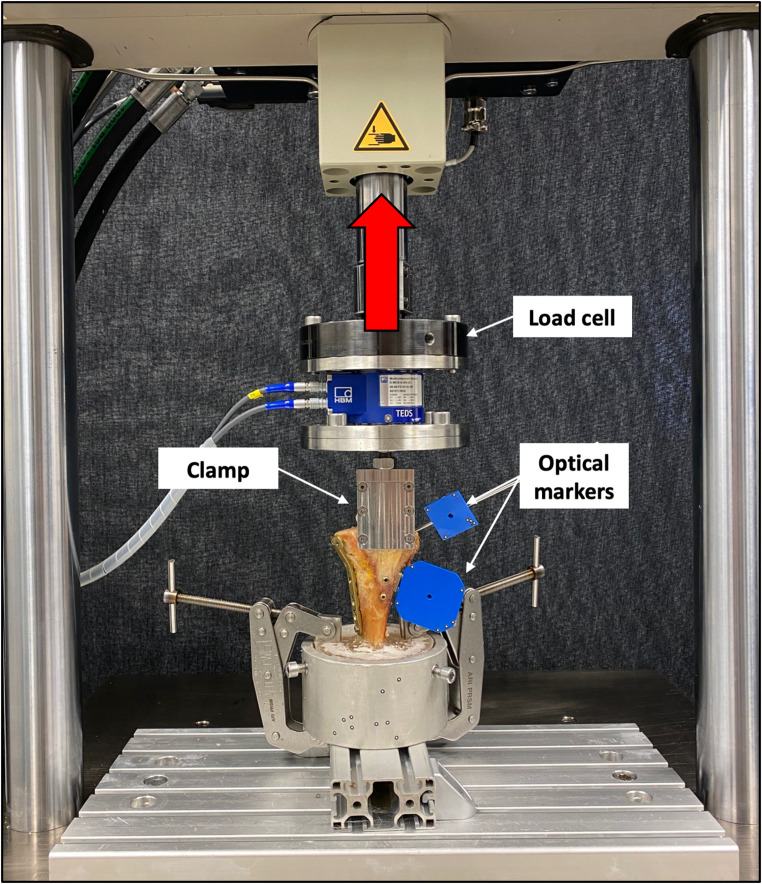
Methods: Two different types of apoepiphyseal tibial tubercle avulsion fractures were created in 40 proximal tibiae according to the modified Ogden classification: (1) Ogden type IIIA and (2) Ogden type IV. The fractures were fixed with either isolated apophyseal screws or additionally with a medial plate or epiphyseal screws. All specimens were biomechanically tested under progressively increasing cyclic loading until failure, while capturing the interfragmentary movements with motion tracking.
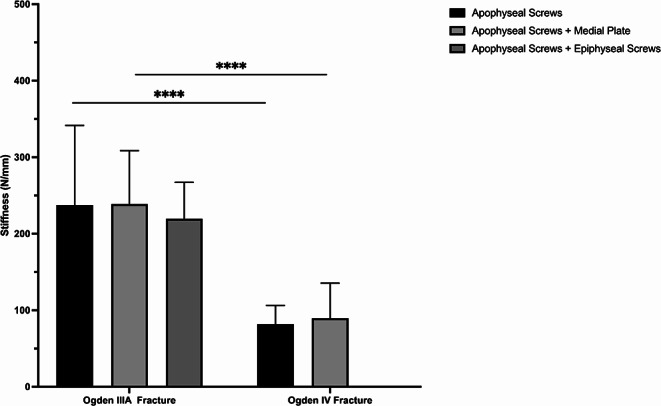
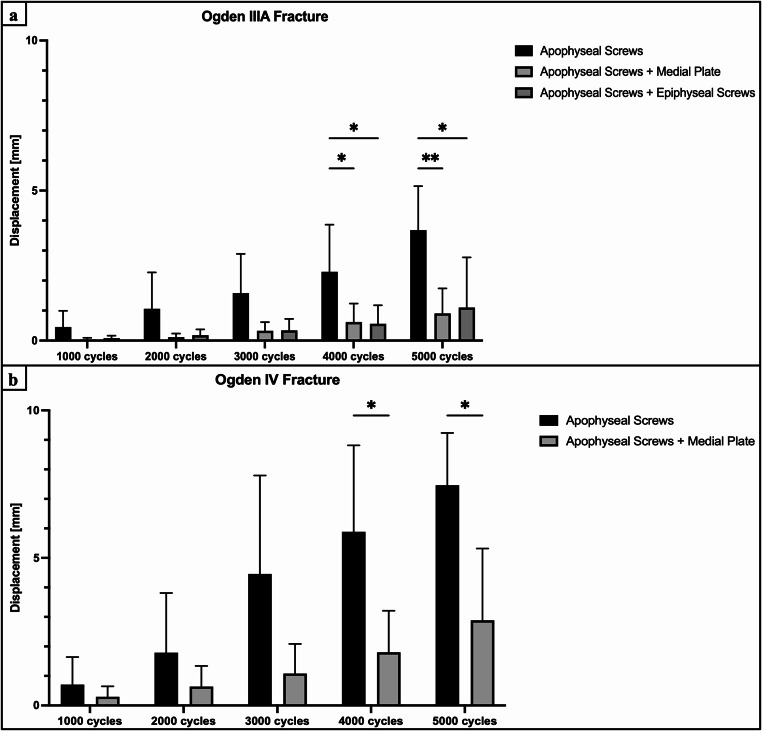
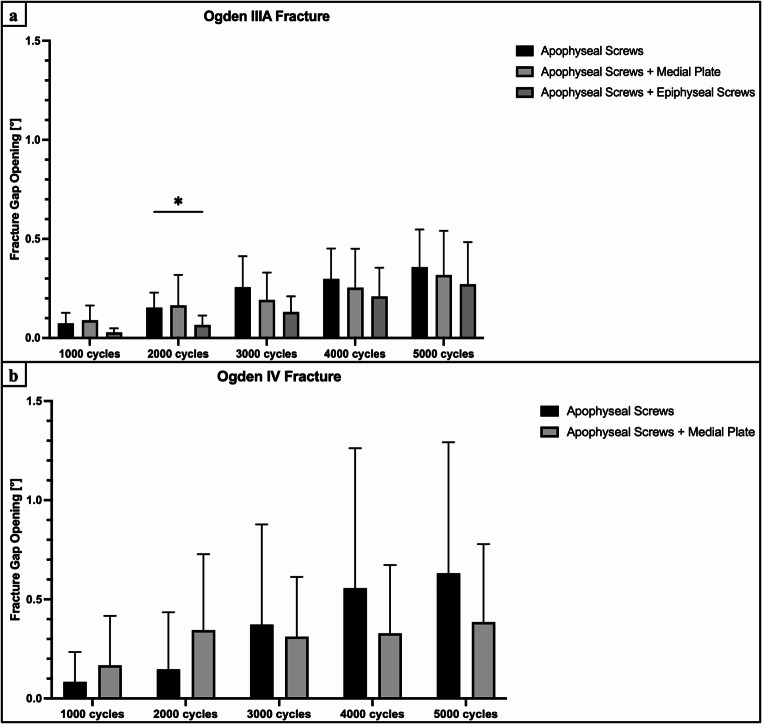
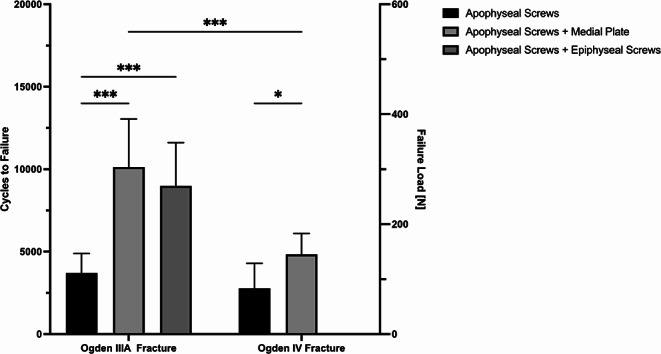
Results: Augmentation of apophyseal screw osteosynthesis by a medial plate in Ogden IV fractures or epiphyseal screws in Ogden IIIA fractures exhibited significantly higher cycles to failure and failure loads (P< 0.05), and significantly less axial displacement (P < 0.05) compared to isolated apophyseal screw fixation. Fixation of Ogden type IIIA fractures resulted in significantly less axial displacements and higher construct stiffness, cycles to failure and failure loads compared to Ogden type IV fracture (P < 0.001). Fracture gap opening did not differ significantly between the fixation techniques.
Conclusions: Augmented apophyseal screw fixation of apoepiphyseal tibial tubercle avulsion fractures provides greater biomechanical stability than isolated apophyseal screw fixation. Regardless of fixation technique, Ogden type IV fractures are more unstable than Ogden type IIIA fractures, so an individualized treatment strategy based on fracture morphology is crucial. In case of an Ogden type IIIA or Ogden type IV fracture, surgeons should consider adding epiphyseal screws or a medial plate osteosynthesis to apophyseal screw fixation to best neutralize forces of the extensor mechanism, as long as the often compromised soft tissue envelope can tolerate greater surgical invasiveness.
Keywords: Biomechanics; Fracture type-specific fixation; Ogden fracture; Tibial tubercle avulsion fracture.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval: The donors gave informed consent to the use of their corpse in medical science during their lifetime. The specimens were dissected and biomechanically tested under the necessary permission from the institutional review board of the AO Research Institute Davos (PP2115, 6 February 2018). Level of evidence: There is no level of evidence as this study was an experimental laboratory study. Competing interests: The authors declare no competing interests.
Figures
References
-
- Bolesta MJ, Fitch RD. Tibial tubercle avulsions. J Pediatr Orthop. 1986;6(2):186–92. 10.1097/01241398-198603000-00013. - PubMed
-
- Hamilton SW, Gibson PH. Simultaneous bilateral avulsion fractures of the tibial tuberosity in adolescence: A case report and review of over 50 years of literature. Knee. 2006;13(5):404–7. 10.1016/j.knee.2006.04.008. - PubMed
-
- Pretell-Mazzini J, Kelly DM, Sawyer JR, Esteban EM, Spence DD, Warner WC Jr., Beaty JH. Outcomes and complications of tibial tubercle fractures in pediatric patients: A systematic review of the literature. J Pediatr Orthop. 2016;36(5):440–6. 10.1097/bpo.0000000000000488. - PubMed
-
- Kalifis G, Marin Fermin T, Seil R, Hobson S, Papakostas E, Hantes M. Tibial tubercle fractures are sports injuries in male adolescents with a considerable risk of complications and reoperations: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2023;31(7):2624–34. 10.1007/s00167-023-07322-1. - PubMed
-
- Pandya NK, Edmonds EW, Roocroft JH, Mubarak SJ. Tibial tubercle fractures: complications, classification, and the need for intra-articular assessment. J Pediatr Orthop. 2012;32(8):749–59. 10.1097/BPO.0b013e318271bb05. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
