

Early rheumatoid arthritis, two distinctive structural damage patterns revealed by MRI: an 8-year longitudinal study
- PMID: 40102269
- PMCID: PMC12350573
- DOI: 10.1007/s00330-025-11493-5
Early rheumatoid arthritis, two distinctive structural damage patterns revealed by MRI: an 8-year longitudinal study
Abstract
Objective: To determine how inflammatory and structural parameters change long-term on standard treatment in rheumatoid arthritis patients and which baseline parameter best predicts long-term structural damage.
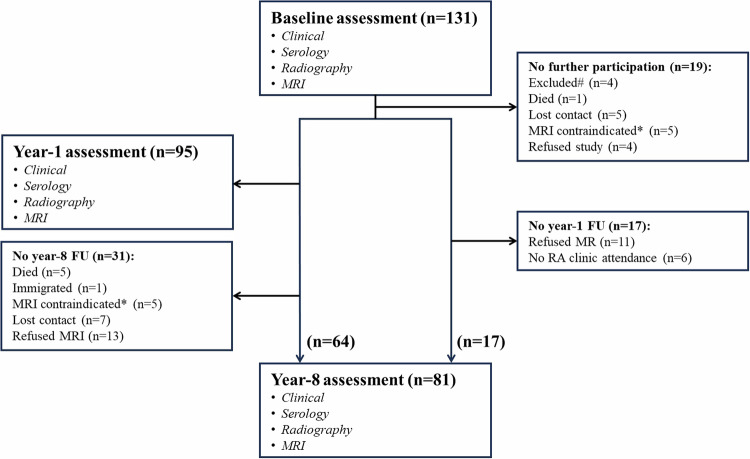
Material and methods: Prospective study of early rheumatoid arthritis (ERA) patients (symptom duration ≤ 24 months) who underwent identical clinical, serological, radiographic, and dynamic contrast-enhanced MRI of the wrist assessments at baseline, year-1, and year-8. MR images were analyzed semi-quantitatively (Rheumatoid Arthritis Magnetic Resonance Imaging Score [RAMRIS]) and quantitatively (synovial volume (cm3); synovial perfusion; bone marrow edema (BME) proportion [%]). Multivariate analyses and receiver operating curves were applied to find the best predictor of long-term structural damage.
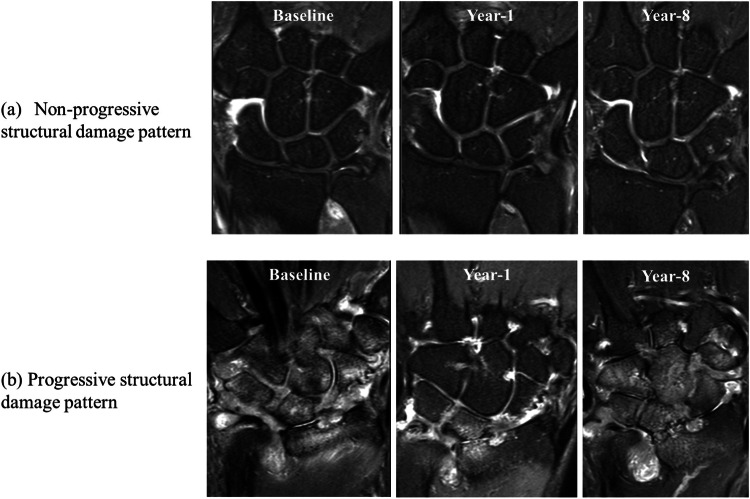
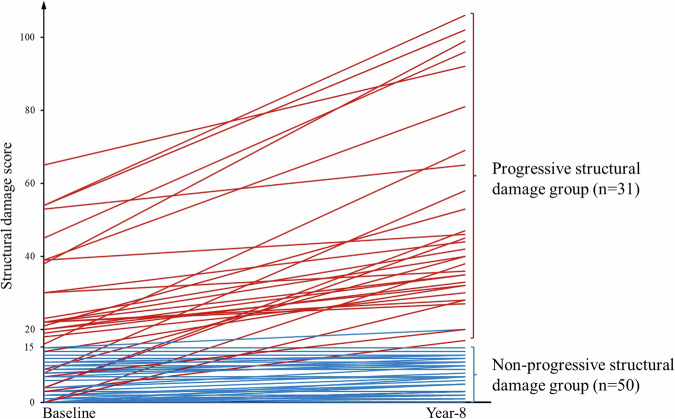
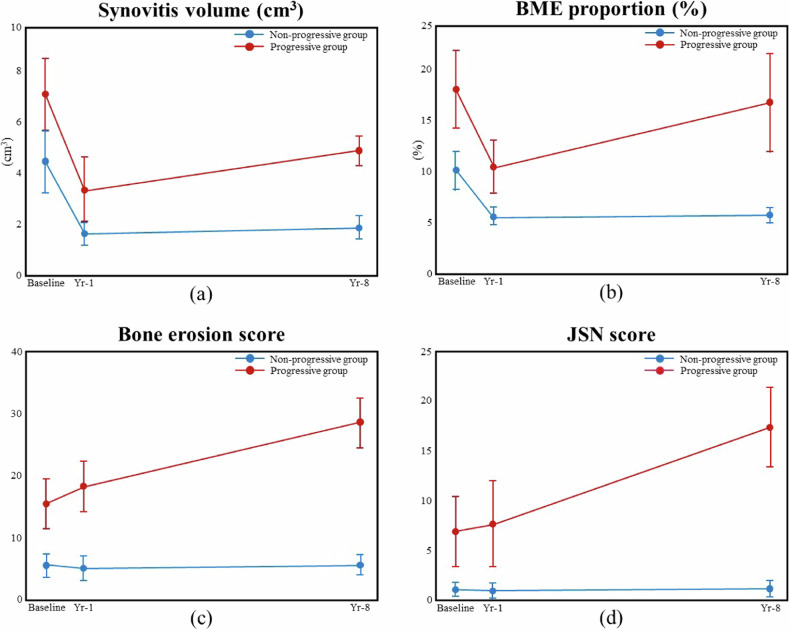
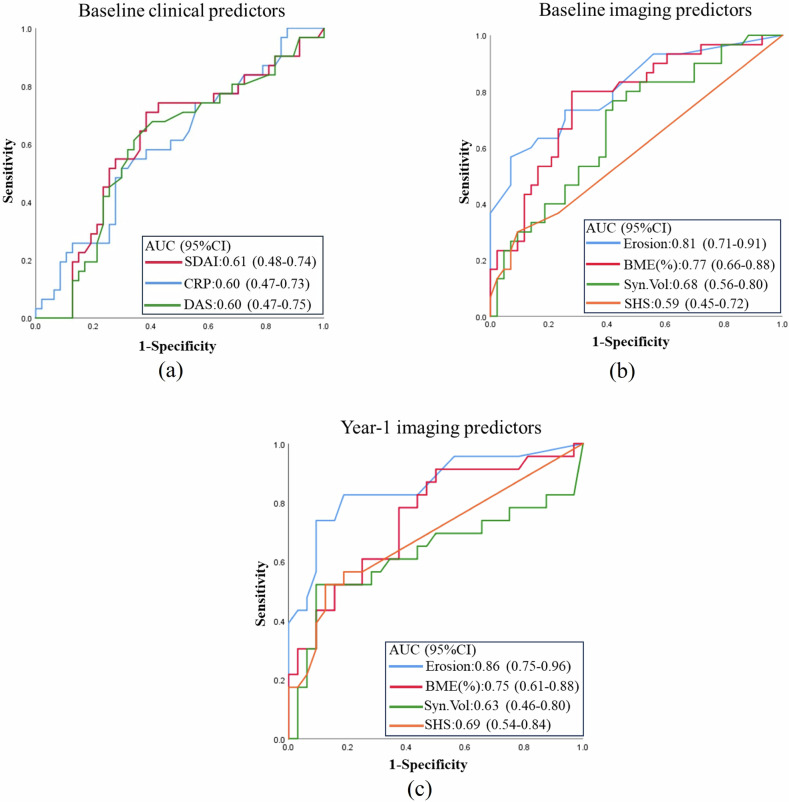
Results: 81 patients (61 ± 12 years, F/M:67/14) were studied. MRI-detected inflammatory parameters markedly improved from baseline to year-1 and slightly deteriorated from year-1 to year-8 (synovial volume:6.7 ± 5.0→2.6 ± 2.9→3.6 ± 3.3 cm3 (p < 0.01); BME proportion:13.1 ± 9.3→7.4 ± 5.0→9.2 ± 9.7% [p < 0.01]). Structural damage progressively deteriorated from baseline to year-8. Two long-term structural damage pattern groups were apparent, namely a "non-progressive structural damage pattern" (62%, 50/81) and a "progressive structural damage pattern" (38%, 31/81). Functional impairment was more frequent and more severe at year-8 in patients with progressive structural damage. MRI-detected bone erosion score better predicted (AUC = 0.81, CI: 0.71-0.91) year-8 structural damage than clinical (SDAI AUC = 0.61, CI: 0.48-0.74), serological (CRP AUC = 0.60, CI: 0.47-0.73), or radiographic (AUC = 0.59, CI: 0.45-0.72) assessment.
Conclusion: In ERA patients, two distinct structural damage patterns are evident. Baseline bone erosion score is better than clinical, serological, or radiographic assessment at predicting long-term structural damage.
Key points: Questions The value of MRI in predicting long-term structural damage in ERA patients is not clear. Findings This study identified two distinct long-term structural damage progression patterns of ERA patients. MRI can better differentiate between these two groups at baseline than clinical, serological, or radiographic assessment. Clinical relevance MRI examination should be performed in all ERA patients at baseline to determine their structural damage pattern. This will allow a better prediction of patient outcomes in the long-term.
Keywords: Follow-up study; MRI; Synovitis; Wrist, Rheumatoid arthritis.
© 2025. The Author(s).
Conflict of interest statement
Compliance with ethical standards. Guarantor: The scientific guarantor of this publication is James F. Griffith. Conflict of interest: The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article. Statistics and biometry: Jason Leung kindly provided statistical advice for this manuscript. Informed consent: Written informed consent was obtained from all subjects (patients) in this study. Ethical approval: This study only involves human participants. This study was approved by the Clinical Research Ethics Committee of the Joint Chinese University of Hong Kong (CUHK) and New Territories East Cluster (NTEC) (Ref. No.: 2021.398). Participants gave informed consent to participate in the study before taking part. Study subjects or cohorts overlap: Some of the baseline to 1-year follow-up results of this study patients were published previously. This prior study addressed changes at baseline and year-1 in 77 of the initial cohort of patients included in the current study. The current study expanded the baseline cohort with the recruitment of more patients and followed up this larger baseline cohort for 8 years. Xiao et al [9] A section of this study on patients also overlaps with this published study. Fifty ERA patients were randomly selected at baseline and year -1 to develop a program to automatically segment the wrist bones and calculate BME proportion (%) and BME relative intensity. This program is used in the current study as a quantification method for BME. Yiu et al [15]. Methodology: Prospective Observational Performed at one institution
Figures
References
-
- Buch MH, Eyre S, McGonagle D (2021) Persistent inflammatory and non-inflammatory mechanisms in refractory rheumatoid arthritis. Nat Rev Rheumatol 17:17–33 - PubMed
-
- Aletaha D, Smolen JS (2018) Diagnosis and management of rheumatoid arthritis: a review. JAMA 320:1360–1372 - PubMed
-
- Smolen JS, Aletaha D, McInnes IB (2016) Rheumatoid arthritis. (published correction appears in Lancet 22:388 (1984)). Lancet 388:2023–2038 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
