

Wearable data reveals distinct characteristics of individuals with persistent symptoms after a SARS-CoV-2 infection
- PMID: 40102642
- PMCID: PMC11920215
- DOI: 10.1038/s41746-025-01456-x
Wearable data reveals distinct characteristics of individuals with persistent symptoms after a SARS-CoV-2 infection
Abstract
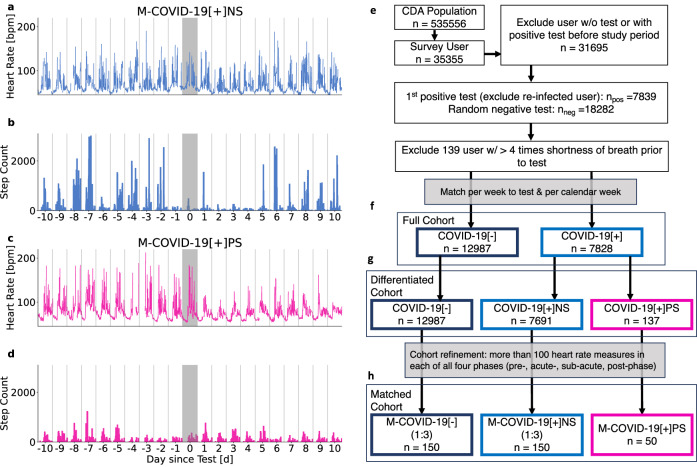
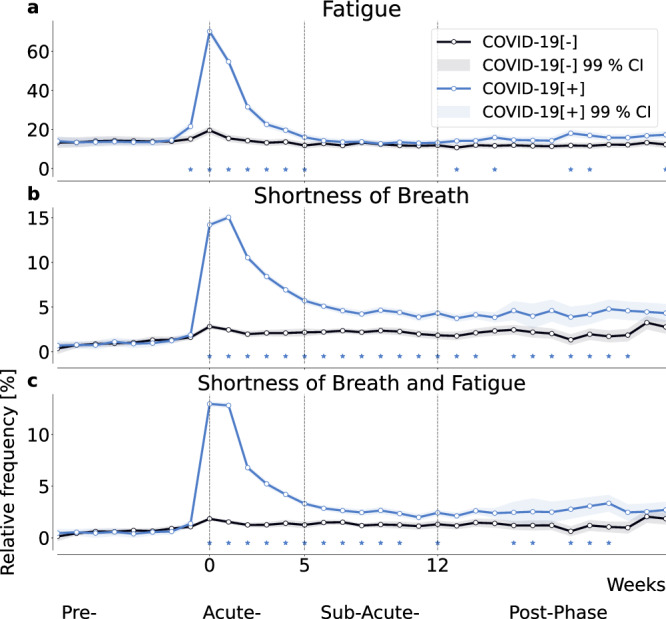
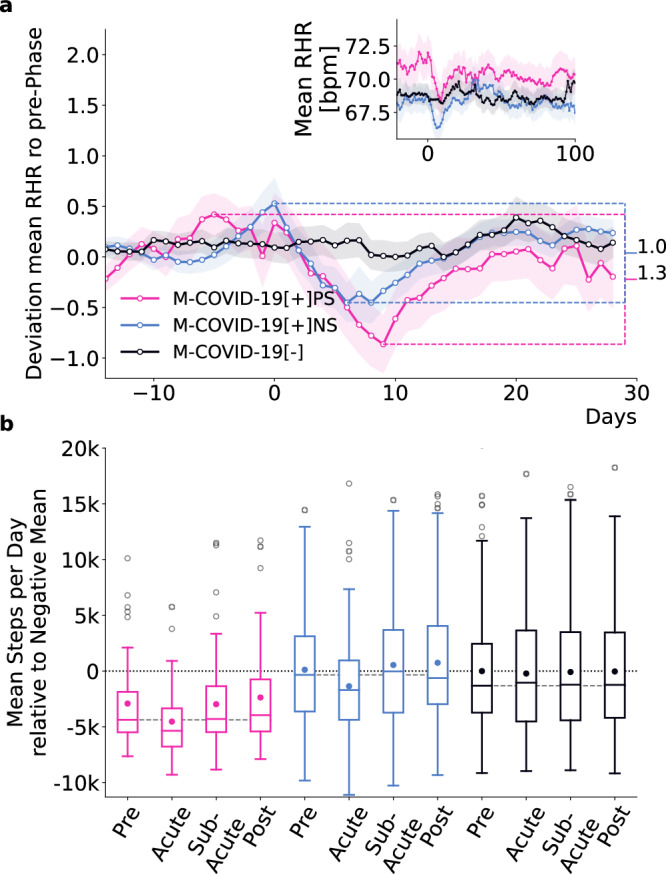
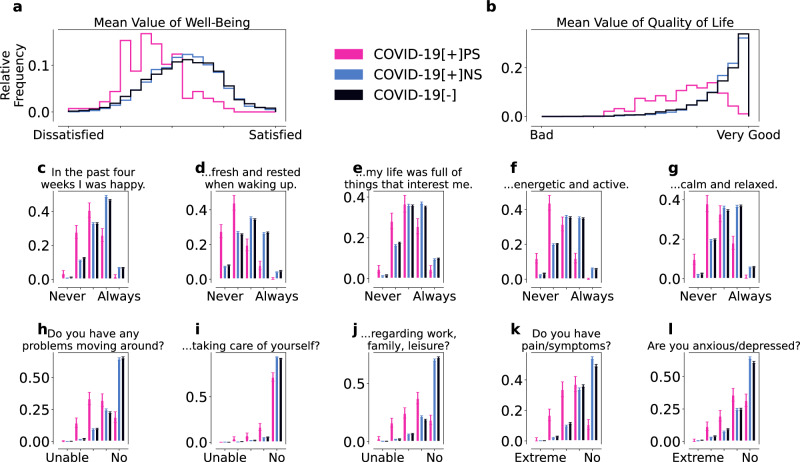
Understanding the factors associated with persistent symptoms after SARS-CoV-2 infection is critical to improving long-term health outcomes. Using a wearable-derived behavioral and physiological dataset (n = 20,815), we identified individuals characterized by self-reported persistent fatigue and shortness of breath after SARS-CoV-2 infection. Compared with symptom-free COVID-19 positive (n = 150) and negative controls (n = 150), these individuals (n = 50) had higher resting heart rates (mean difference 2.37/1.49 bpm) and lower daily step counts (mean 3030/2909 steps fewer), even at least three weeks prior to SARS-CoV-2 infection. In addition, persistent fatigue and shortness of breath were associated with a significant reduction in mean quality of life (WHO-5, EQ-5D), even before infection. Here we show that persistent symptoms after SARS-CoV-2 infection may be associated with pre-existing lower fitness levels or health conditions. These findings additionally highlight the potential of wearable devices to track health dynamics and provide valuable insights into long-term outcomes of infectious diseases.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Factors Associated with Long Covid Symptoms in an Online Cohort Study.medRxiv [Preprint]. 2022 Dec 6:2022.12.01.22282987. doi: 10.1101/2022.12.01.22282987. medRxiv. 2022. Update in: Open Forum Infect Dis. 2023 Feb 01;10(2):ofad047. doi: 10.1093/ofid/ofad047. PMID: 36523412 Free PMC article. Updated. Preprint.
-
A Prospective Study of Patients with Persistent Symptoms after SARS-CoV-2 Infection Referred to Physical Medicine and Rehabilitation.Acta Med Port. 2023 Oct 2;36(10):639-646. doi: 10.20344/amp.19382. Epub 2023 Jul 18. Acta Med Port. 2023. PMID: 37466050
-
Estimated Global Proportions of Individuals With Persistent Fatigue, Cognitive, and Respiratory Symptom Clusters Following Symptomatic COVID-19 in 2020 and 2021.JAMA. 2022 Oct 25;328(16):1604-1615. doi: 10.1001/jama.2022.18931. JAMA. 2022. PMID: 36215063 Free PMC article.
-
Assessment of the Frequency and Variety of Persistent Symptoms Among Patients With COVID-19: A Systematic Review.JAMA Netw Open. 2021 May 3;4(5):e2111417. doi: 10.1001/jamanetworkopen.2021.11417. JAMA Netw Open. 2021. PMID: 34037731 Free PMC article.
-
Persistent symptoms following SARS-CoV-2 infection amongst children and young people: A meta-analysis of controlled and uncontrolled studies.J Infect. 2022 Feb;84(2):158-170. doi: 10.1016/j.jinf.2021.11.011. Epub 2021 Nov 20. J Infect. 2022. PMID: 34813820 Free PMC article.
References
-
- World Health Organization. Post COVID-19 condition (Long COVID). https://www.who.int/europe/news-room/fact-sheets/item/post-covid-19-cond....
LinkOut - more resources
Full Text Sources
Miscellaneous
