

Impact of tracheostomy on clinical outcomes in ventilated patients with severe pneumonia: a propensity-matched cohort study
- PMID: 40102711
- PMCID: PMC11938709
- DOI: 10.3904/kjim.2024.248
Impact of tracheostomy on clinical outcomes in ventilated patients with severe pneumonia: a propensity-matched cohort study
Abstract
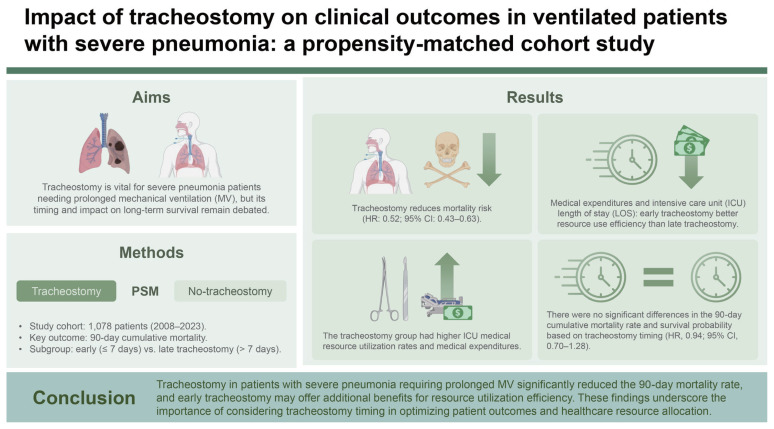
Background/aims: Tracheostomy is a crucial intervention for severe pneumonia patients requiring prolonged mechanical ventilation (MV). However, debate persists regarding the influence of tracheostomy timing and performance on long-term survival outcomes. This study utilized propensity score matching to assess the impact of tracheostomy timing and performance on patient survival outcomes.
Methods: A retrospective observational study employing propensity score matching was conducted of respiratory intensive care unit (ICU) patients who underwent prolonged acute MV due to severe pneumonia from 2008 to 2023. The primary outcome was the 90-day cumulative mortality rate, with secondary outcomes including ICU medical resource utilization rates.
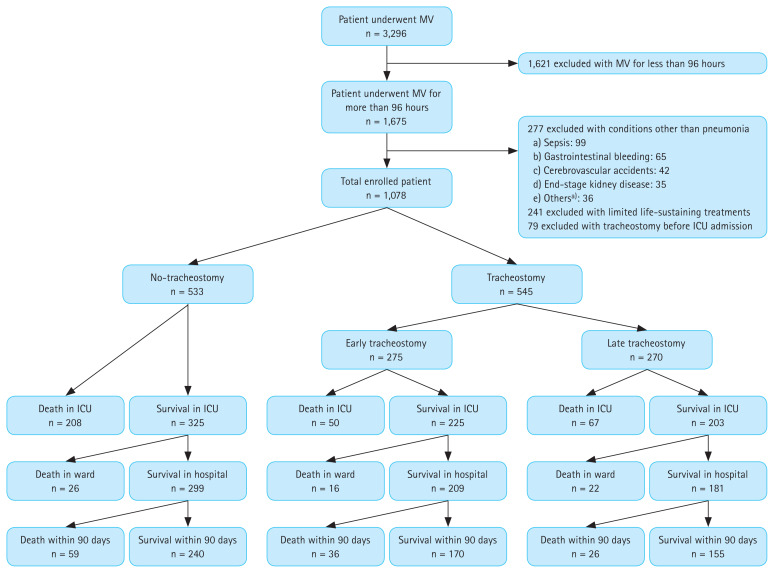
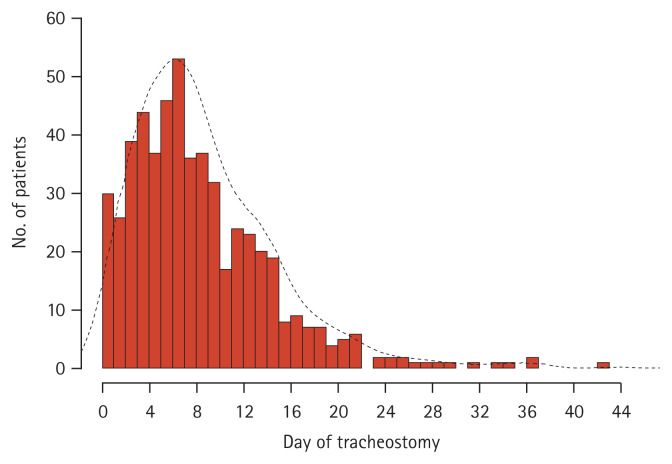
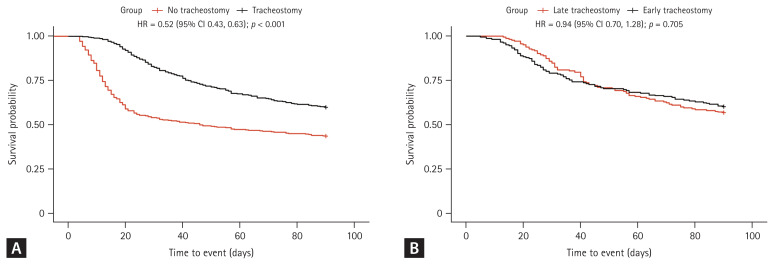
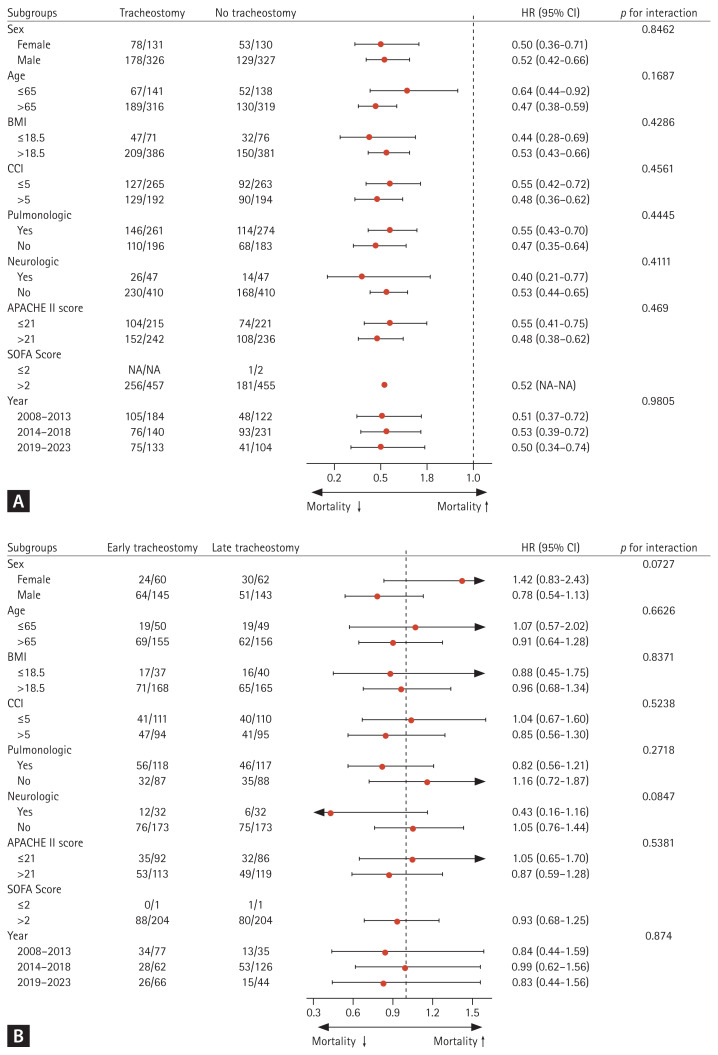
Results: Out of 1,078 patients, 545 underwent tracheostomy with a median timing of 7 days. The tracheostomy group exhibited lower 90-day cumulative mortality and a higher survival probability (hazard ratio [HR] 0.52, 95% confidence interval [CI] 0.43-0.63) than the no-tracheostomy group. The tracheostomy group had higher ICU medical resource utilization rates and medical expenditures. The early tracheostomy group (≤ 7 days) had lower ICU medical resource utilization rates and medical expenditures than the late tracheostomy group (> 7 days). However, there were no significant differences in the 90-day cumulative mortality rate and survival probability based on tracheostomy timing (HR 0.94, 95% CI 0.70-1.28).
Conclusion: Tracheostomy in patients with severe pneumonia requiring prolonged MV significantly reduced the 90-day mortality rate, and early tracheostomy may offer additional benefits for resource utilization efficiency. These findings underscore the importance of considering tracheostomy timing in optimizing patient outcomes and healthcare resource allocation.
Keywords: Mechanical ventilation; Mortality; Pneumonia; Propensity score; Tracheostomy.
Conflict of interest statement
The authors disclose no conflicts.
Figures
Similar articles
-
Comparison of Outcomes Between Early and Late Tracheostomy.Respir Care. 2023 Dec 28;69(1):76-81. doi: 10.4187/respcare.10837. Respir Care. 2023. PMID: 37468334 Free PMC article.
-
Is tracheostomy associated with better outcomes for patients requiring long-term mechanical ventilation?Crit Care Med. 2007 Mar;35(3):802-7. doi: 10.1097/01.CCM.0000256721.60517.B1. Crit Care Med. 2007. PMID: 17255861
-
Association of timing of tracheostomy on clinical outcomes in PICU patients.Pediatr Crit Care Med. 2015 Mar;16(3):e52-8. doi: 10.1097/PCC.0000000000000336. Pediatr Crit Care Med. 2015. PMID: 25581633
-
Early Versus Late Tracheostomy in Patients With Acute Traumatic Spinal Cord Injury: A Systematic Review and Meta-analysis.Anesth Analg. 2021 Feb 1;132(2):384-394. doi: 10.1213/ANE.0000000000005212. Anesth Analg. 2021. PMID: 33009136
-
Early tracheostomy in intensive care trauma patients improves resource utilization: a cohort study and literature review.Crit Care. 2004 Oct;8(5):R347-52. doi: 10.1186/cc2924. Epub 2004 Aug 23. Crit Care. 2004. PMID: 15469579 Free PMC article. Review.
References
-
- Fagon JY, Chastre J, Vuagnat A, Trouillet JL, Novara A, Gibert C. Nosocomial pneumonia and mortality among patients in intensive care units. JAMA. 1996;275:866–869. - PubMed
-
- Holzapfel L, Chevret S, Madinier G, et al. Influence of long-term oro- or nasotracheal intubation on nosocomial maxillary sinusitis and pneumonia: results of a prospective, randomized, clinical trial. Crit Care Med. 1993;21:1132–1138. - PubMed
-
- Freeman BD. Tracheostomy update: when and how. Crit Care Clin. 2017;33:311–322. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical