

Rural hospital incident command leaders' perceptions of disaster preparedness
- PMID: 40102726
- PMCID: PMC11921675
- DOI: 10.1186/s12873-025-01201-3
Rural hospital incident command leaders' perceptions of disaster preparedness
Abstract
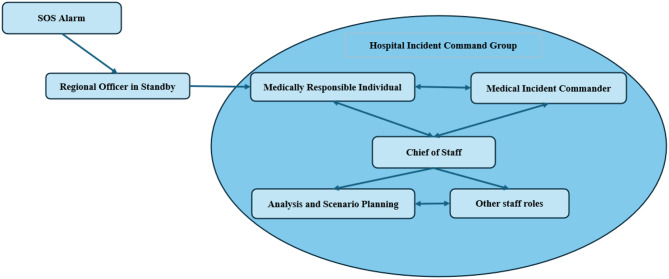
Background: Recent trends indicate that the frequency of major incidents (MIs) is increasing. Healthcare systems are vital actors in societies' responses to MIs. Well-prepared healthcare systems may mitigate the effects of MIs. Disaster preparedness is based on region-specific risk and vulnerability analyses (RVAs). Hospital incident command groups (HICGs) are commonly formed per hospital's contingency plan MI to aid in disaster response. Acquiring situational awareness and decision-making in the face of uncertainty are known challenges for HICGs during MIs. However, the remoteness of rural hospitals presents unique challenges.
Aim: The aim of this study was to explore HICG leaders' perceptions of disaster preparedness in rural hospitals.
Methods: A qualitative study with semi-structured, focus group, and individual interviews was used. The data were analyzed through inductive content analysis.
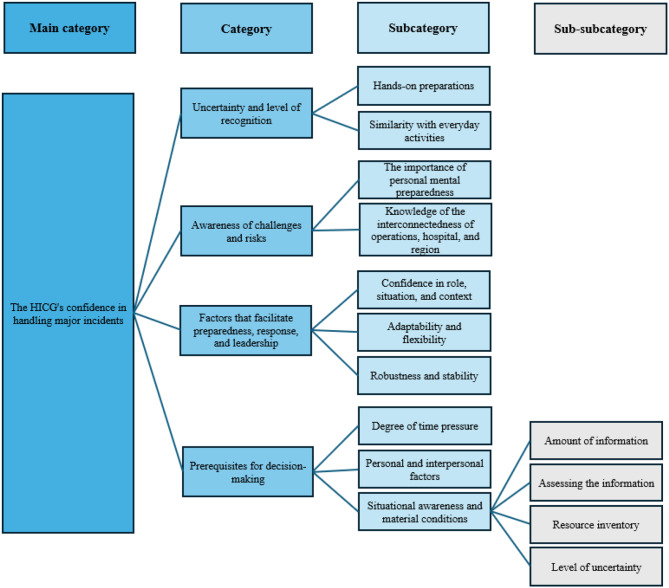
Results: The analysis generated the main category, HICGs' confidence in handling major incidents and four categories. These were Uncertainty and level of recognition (containing two subcategories); Awareness of challenges and risks (containing two subcategories); Factors that facilitate preparedness, response, and leadership (containing three subcategories); and Prerequisites for decision-making (containing three subcategories and four subcategories).
Conclusions: HICG leaders generally perceived their hospital's disaster preparedness as adequate. However, preparedness was found to be influenced by several factors. The findings revealed a complex interplay of factors influencing preparedness and response, particularly highlighting challenges related to geographical isolation and resource constraints. Effective preparedness requires a comprehensive understanding of local contexts, hospital capabilities, and risks, which directly impacts training, decision-making, and resource allocation. Addressing the identified vulnerabilities necessitates targeted interventions focused on situational awareness, decision-making, collaboration, and training.
Clinical trial number: Not applicable.
Keywords: Decision-making; Disaster medicine; Disaster preparedness; Hospital incident command; Major incident; Rural preparedness.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: The study was approved by the “Ethical Review and Personal Data Management” at the faculty of medicine, Department of Diagnostics and Intervention, Umeå University. The participants participated in their professional functions. Neither sensitive personal data nor personal data about violations of law were gathered. In addition, this study did not employ a method that would have a negative psychological impact on the participants. The data presented were coded and anonymized, ensuring anonymity. The participants were informed of the aim of the study and guaranteed anonymity and confidentiality concerning the data produced in this study. Written consent was obtained from all participants, and the participants were informed that they could withdraw from the study without consent. Principles, as stated by the Declaration of Helsinki and the Swedish Regional Ethics Committee, regarding ethics were followed [39, 40]. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Does the "state of disaster" response have a downside? Hospital incident command group leaders' experiences of a terrorist-induced major incident: a qualitative study.BMC Emerg Med. 2025 Feb 4;25(1):21. doi: 10.1186/s12873-025-01173-4. BMC Emerg Med. 2025. PMID: 39901074 Free PMC article.
-
Registered nurses' experience as disaster preparedness coordinators during a major incident: A qualitative study.Nurs Open. 2022 Jan;9(1):329-338. doi: 10.1002/nop2.1066. Epub 2021 Sep 21. Nurs Open. 2022. PMID: 34546003 Free PMC article.
-
Exploring hospitals' functional preparedness effective factors in response to disasters: a qualitative study in a lower middle-income country.BMC Health Serv Res. 2024 Feb 13;24(1):197. doi: 10.1186/s12913-024-10630-y. BMC Health Serv Res. 2024. PMID: 38350908 Free PMC article.
-
The Role of Hospital Medicine in Emergency Preparedness: A Framework for Hospitalist Leadership in Disaster Preparedness, Response, and Recovery.J Hosp Med. 2018 Sep;13(10):713-718. doi: 10.12788/jhm.3073. J Hosp Med. 2018. PMID: 30261086 Review.
-
Leadership and hospital preparedness: disaster management and emergency services in pediatrics.J Trauma. 2009 Aug;67(2 Suppl):S79-83. doi: 10.1097/TA.0b013e3181af069f. J Trauma. 2009. PMID: 19667858 Review.
References
-
- Centre for Research on the Epidemiology of Disasters. 2023: Disasters in Numbers. 2024.
-
- World Health Organization. A strategic framework for emergency preparedness. Geneva, Switzerland; 2017.
-
- Chuang S, Woods DD, Ting HW, Cook RI, Hsu JC. Coping with a mass casualty: Insights into a hospital's emergency response and adaptations after the Formosa Fun Coast Dust Explosion. Disaster Med Public Health Preparedness. 2020;14(4):467-76. - PubMed
-
- Hasan MK, Nasrullah SM, Quattrocchi A, Arcos González P, Castro-Delgado R. Hospital surge capacity preparedness in disasters and emergencies: a systematic review. Public Health. 2023;225:12-21. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
