

Sample size recalculation based on the overall success rate in a randomized test-treatment trial with restricting randomization to discordant pairs
- PMID: 40102729
- PMCID: PMC11921670
- DOI: 10.1186/s12874-024-02410-3
Sample size recalculation based on the overall success rate in a randomized test-treatment trial with restricting randomization to discordant pairs
Abstract
Background: Randomized test-treatment studies are performed to evaluate the clinical effectiveness of diagnostic tests by assessing patient-relevant outcomes. The assumptions for a sample size calculation for such studies are often uncertain.
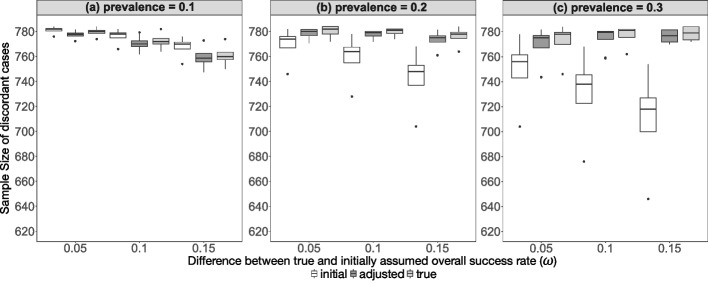
Methods: An adaptive design with a blinded sample size recalculation based on the overall success rate in a randomized test-treatment trial with restricting randomization to discordant pairs is proposed and evaluated by a simulation study. The results of the adaptive design are compared to those of the fixed design.
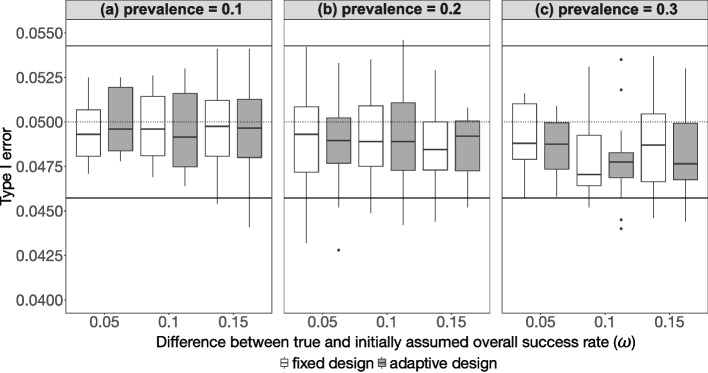
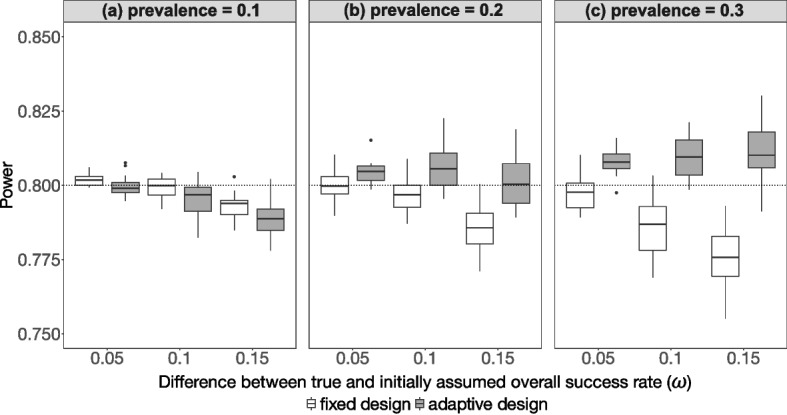
Results: The empirical type I error rate is sufficiently controlled in the adaptive design as well as in the fixed design and the estimates are unbiased. The adaptive design achieves the desired theoretical power, whereas the fixed design tends to be over- or under-powered.
Conclusions: It may be advisable to consider blinded recalculation of sample size in a randomized test-treatment study with restriction of randomization to discordant pairs in order to improve the conduct of the study. However, there are a number of study-related limitations that affect the implementation of the method which need to be considered.
Keywords: Adaptive design; Diagnostic test; Discordance design; Overall success rate; Sample size recalculation.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Sample size recalculation based on the prevalence in a randomized test-treatment study.BMC Med Res Methodol. 2022 Jul 25;22(1):205. doi: 10.1186/s12874-022-01678-7. BMC Med Res Methodol. 2022. PMID: 35879675 Free PMC article.
-
Sample size recalculation in multicenter randomized controlled clinical trials based on noncomparative data.Biom J. 2020 Sep;62(5):1284-1299. doi: 10.1002/bimj.201900138. Epub 2020 Mar 4. Biom J. 2020. PMID: 32128868
-
A Bayesian sequential design with adaptive randomization for 2-sided hypothesis test.Pharm Stat. 2017 Nov;16(6):451-465. doi: 10.1002/pst.1830. Epub 2017 Oct 4. Pharm Stat. 2017. PMID: 28980435
-
Re-randomization tests in clinical trials.Stat Med. 2019 May 30;38(12):2292-2302. doi: 10.1002/sim.8093. Epub 2019 Jan 22. Stat Med. 2019. PMID: 30672002 Review.
-
A New Statistical Method for Designing Stepped-Wedge Cluster Trials [Internet].Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2022 May. Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2022 May. PMID: 39666843 Free Books & Documents. Review.
References
-
- Committee for Medicinal Products for Human Use (CHMP). Guideline on Clinical Evaluation of Diagnostic Agents. European Medicines Agency. 2009. Available from: https://www.ema.europa.eu/en/document. https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-cl....
-
- Pepe MS. The statistical evaluation of medical tests for classification and prediction. Oxford university press; 2003.
-
- Lijmer JG, Bossuyt PMM. Various randomized designs can be used to evaluate medical tests. J Clin Epidemiol. 2009Apr;62(4):364–73. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
