

The impact of inter-hospital transfer on outcomes in lower gastrointestinal bleeding: a retrospective cohort analysis
- PMID: 40102773
- PMCID: PMC11917058
- DOI: 10.1186/s12876-025-03755-9
The impact of inter-hospital transfer on outcomes in lower gastrointestinal bleeding: a retrospective cohort analysis
Abstract
Background: This study investigates the role of interhospital transfer (IHT) in lower gastrointestinal bleeding (LGIB) management and its impact on patient outcomes, focusing on mortality rates, complication occurrences, procedural performance, and resource utilization in patients diagnosed with LGIB.
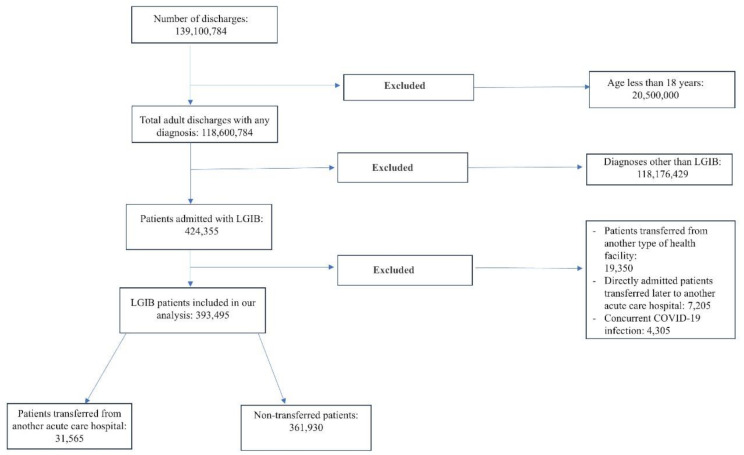
Methods: This retrospective cohort study used data from the National Inpatient Sample database from 2017 to 2020. It included adult patients diagnosed with LGIB, assessing the impact of IHT on outcomes such as mortality, complication rates, procedural performance, and resource utilization. Adjusted odds ratios (AOR) and adjusted mean differences (AMD) were used to evaluate these impacts.
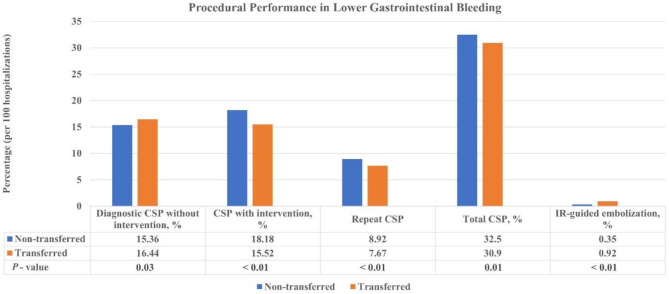
Results: A total of 393,495 LGIB patients were analyzed, with 31,565 (8.02%) undergoing interhospital transfer. Transferred patients exhibited significantly higher inpatient mortality (AOR 1.96, P < 0.01). They also faced increased risks of acute kidney injury (AOR 1.32, P < 0.01), septic shock (AOR 2.11, P < 0.01), and intensive care unit admission (AOR: 2.61, P < 0.01). These patients were more likely to undergo interventional radiology-guided embolization (AOR 2.68, P < 0.01) and showed variations in colonoscopy procedures. Resource utilization was also higher among transferred patients, with an increased mean length of hospital stay by 4.37 days (P < 0.01) and higher hospitalization charges (mean difference $61,239, P < 0.01).
Conclusion: Interhospital transfer in LGIB patients is associated with increased mortality, greater resource utilization, and the need for more specialized procedural interventions. Enhanced clinical vigilance and tailored resource allocation for transferred LGIB patients are necessary. Future research should optimize care strategies for these high-risk patients.
Keywords: Hospitalization; Interhospital transfer; Lower Gastrointestinal bleeding; National inpatient sample; Patient outcomes; Resource utilization.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study did not involve primary data collection from human participants, as it exclusively utilized secondary data from publicly available sources (the National Inpatient Sample Database), which are de-identified and exempt from requiring ethical approval. While ethical approval for the use of this dataset was sought by the Office of Human Research Protection Rochester Rochester Health, the study was deemed exempt from full review due to the nature of the data. All research activities were conducted in compliance with relevant ethical guidelines, including the Declaration of Helsinki. Consent for publication: Not applicable. Competing interests: The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- ACG. Lower Gastrointestinal (GI) Bleeding. [cited 2024 Jan 26]. Available from: https://gi.org/topics/lower-gi-bleeding/
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
