

Efficacy of late cervical cerclage for preventing preterm birth in pregnancies complicated by cervical incompetence: retrospective cohort study
- PMID: 40102776
- PMCID: PMC11916929
- DOI: 10.1186/s12884-025-07432-3
Efficacy of late cervical cerclage for preventing preterm birth in pregnancies complicated by cervical incompetence: retrospective cohort study
Abstract
Objectives: To compare different periods of cerclage placement in preventing preterm birth in singleton pregnancies complicated by cervical incompetence.
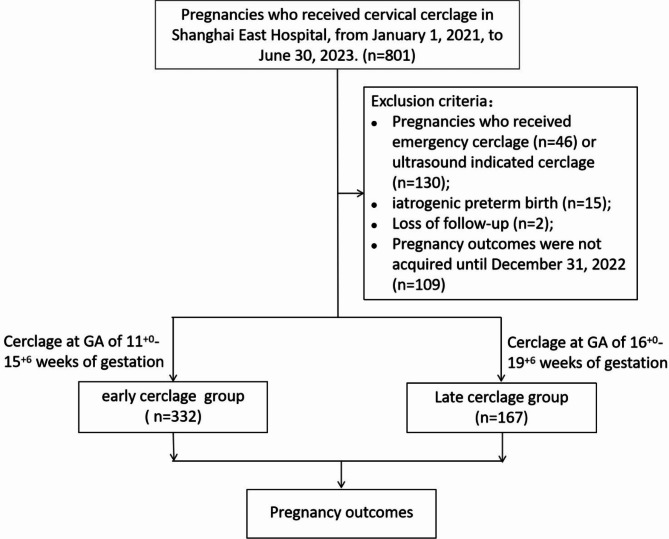
Methods: This retrospective cohort study was conducted at a tertiary hospital in Shanghai, China. A total of 499 singleton pregnancies undergoing prophylactic cervical cerclage between January 1, 2021, and June 30, 2023, at Shanghai East Hospital were included in the study. Participants were classified into the early cerclage group (cerclage performed at 11+ 0 to 15+ 6 weeks of gestation) and the late cerclage group (cerclage performed at 16+ 0 to 19+ 6 weeks of gestation).
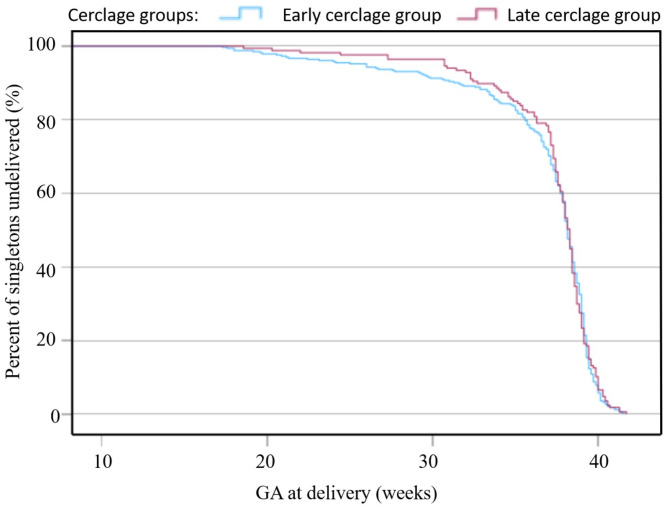
Results: The median gestational ages at delivery were similar between the early cerclage group and the late cerclage group (median (IQR) 38.1 (36.6-39.1) vs. 38.3 (37.1-39.0) weeks, p = 0.568). There was no difference in preterm birth rates of < 37 (28.0%, 93/332 vs. 21.0%, 35/167, p = 0.089), < 34 (14.8%, 49/332 vs. 11.4%, 18/167, p = 0.218), or < 28 (6.9%, 23/332 vs. 3.0%, 5/167, p = 0.072) weeks of gestation between the early cerclage group and the late cerclage group. The incidence rates of chorioamnionitis, premature rupture of membranes, and cesarean section were comparable between the two groups. As a primary indicator of neonatal outcomes, the survival rates of newborns at three months post-delivery were similar between the early and late cerclage groups (94.6%, 314/332 vs. 98.2%, 164/167, p = 0.061). Birth weights of newborns in the early and late cerclage groups were not significantly different (median (IQR) 3080.0 (2652.5-3450.0) vs. 3210.0 (2600.0-3550.0) g, p = 0.100). The incidence rate of 5-minute Apgar scores < 7 in the late cerclage group was significantly lower than that in the early cerclage group (1.8%, 3/167 vs. 6.3%, 21/332, p = 0.026). The incidence rates of neonatal intensive care unit admission, and respiratory distress syndrome were similar between the two groups.
Conclusions: Our retrospective study demonstrated that the efficacy and risk of prophylactic cervical cerclage performed at 16+ 0 to 19+ 6 weeks of gestation were comparable to those of earlier cerclage performed at 11+ 0 to 15+ 6 weeks. Our study provided robust evidence supporting the safety and clinical feasibility of late cerclage in preventing preterm birth, which offers valuable insights into optimizing the cerclage period for high-risk pregnancies.
Keywords: Cervical incompetence; Early cervical cerclage; Late cervical cerclage; Pregnancy outcome; Preterm birth; Singleton; Transvaginal cerclage.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the ethics committee of Shanghai East Hospital (approval number 2019 − 195). Patients included in the study were informed of the risks and potential benefits associated with transvaginal cerclage and provided written informed consent. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- ACOG Practice Bulletin 142. Cerclage for the management of cervical insufficiency. Obstet Gynecol. 2014;123(2 Pt 1):372–9. - PubMed
-
- Shirodkar VN. A new method of operative treatment of habitual abortion. Antiseptic. 1955;52:299.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
