

Evaluating methods to define place of residence in Canadian administrative data and the impact on observed associations with all-cause mortality in type 2 diabetes
- PMID: 40102777
- PMCID: PMC11921607
- DOI: 10.1186/s12874-025-02531-3
Evaluating methods to define place of residence in Canadian administrative data and the impact on observed associations with all-cause mortality in type 2 diabetes
Abstract
Purpose: An individual's location of residence may impact health, however, health services and outcomes research generally use a single point in time to define where an individual resides. While this estimate of residence becomes inaccurate when the study subject moves, the impact on observed associations is not known. This study quantifies the impact of different methods to define residence (rural, urban, metropolitan) on the association with all-cause mortality.
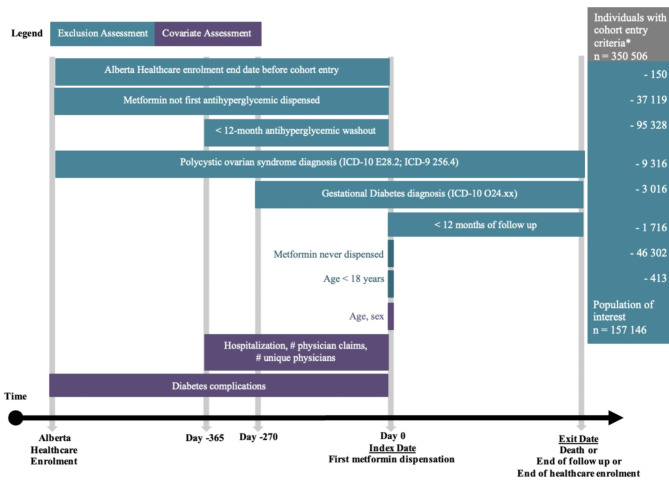
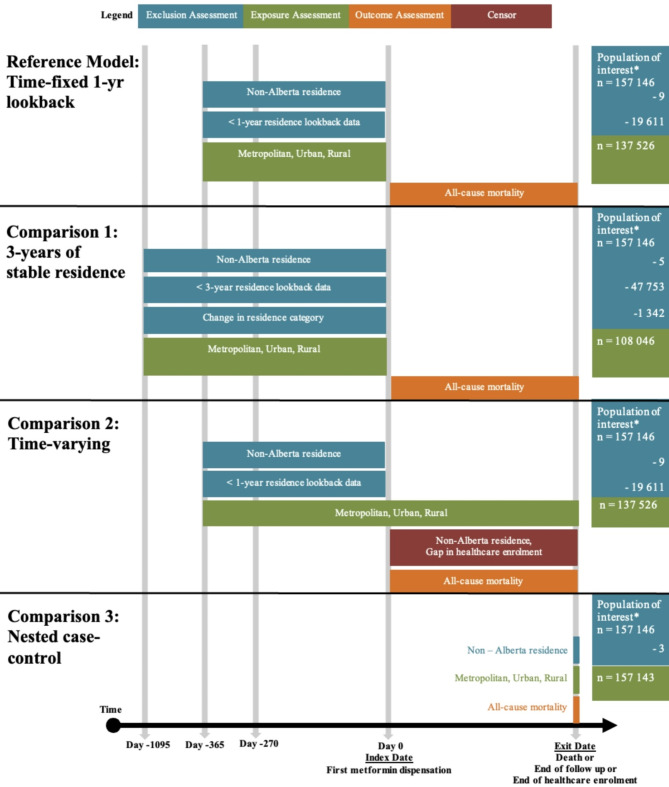
Methods: A diabetes cohort of new metformin users was identified from administrative data in Alberta, Canada between 2008 and 2019. An individual's residence (rural/urban/metropolitan) was defined from postal codes using 4 different methods: residence defined at 1-year before first metformin (this served as the reference model), comparison 1- stable residence for 3 years before first metformin, comparison 2- residence as time-varying (during the outcome observation window), and comparison 3 - nested case control (residence closest to the index date after identifying cases and controls). Multivariable Cox proportional hazard and logistic regression models were constructed to examine the association between residence definitions and all-cause mortality.
Results: We identified 157,146 new metformin users (mean age of 55 years and 57% male) and 8,444 (5%) deaths occurred during the mean follow up of 4.7 (SD 2.3) years. There were few instances of moving after first metformin; 2.6% of individuals moved to a smaller centre (metropolitan to urban or rural, or urban to rural) and 3.1% moved to a larger centre (rural to urban or metropolitan, or urban to metropolitan). The association between rural residence and all-cause mortality was consistent (aHR:1.18; 95%CI:1.12-1.24), regardless of the method used to define residence.
Conclusions: The method used to define residence in a population of adults newly treated with metformin for type 2 diabetes has minimal impact on measures of all-cause mortality, possibly due to infrequent migration. The observed association between residence and mortality is compelling but requires further investigation and more robust analysis.
Keywords: Migration; Nested case-control; Rural-urban continuum; Time-fixed; Time-varying; Type 2 diabetes.
Plain language summary
There is growing evidence describing the impact of where an individual lives on their health. However, most of these studies identify place of residence at a single point in time and do not consider when a person moves. This could result in misclassification, which could over- or underestimate the influence of residence on health outcomes. In this study, residence was defined with 4 different methods: at 1-year before starting metformin for type 2 diabetes; stable residence for 3-years before starting metformin; accounting for changes in residence after being newly treated with metformin for type 2 diabetes; and near the end of the study at death or the end of follow up. The results of this study describe that individuals rarely move after treatment initiation with metformin for type 2 diabetes and that living in a rural area has a higher risk of death from any cause, further investigation into the latter is required.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The University of Alberta Research Ethics Board approved the conduct of this study (Pro00066037). Individual level consent was waved as this study used de-identified administrative health data and disclosure for research purposes followed regulations of the Alberta Health Information Act ( https://open.alberta.ca/publications/h05 ). Consent for publication: Not Applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Are Guideline-concordant Processes of Care Consistent Across the Rural-Urban Continuum? A Retrospective Cohort Study of Adults Newly Treated for Type 2 Diabetes.Can J Diabetes. 2024 Jul;48(5):322-329.e5. doi: 10.1016/j.jcjd.2024.03.007. Epub 2024 Apr 5. Can J Diabetes. 2024. PMID: 38583767
-
Rural Residence Is Associated With a Delayed Trend Away From Sulfonylurea Use for Treatment Intensification of Type 2 Diabetes.Diabetes Care. 2023 Mar 1;46(3):613-619. doi: 10.2337/dc22-1223. Diabetes Care. 2023. PMID: 36637880
-
Examining palliative care program use and place of death in rural and urban contexts: a Canadian population-based study using linked data.Rural Remote Health. 2015 Apr-Jun;15(2):3134. Epub 2015 Jun 24. Rural Remote Health. 2015. PMID: 26103433
-
Impact of Drug Exposure Definitions on Observed Associations in Pharmacoepidemiology Research.J Popul Ther Clin Pharmacol. 2018 Mar 20;25(1):e39-e52. doi: 10.22374/1710-6222.25.1.4. J Popul Ther Clin Pharmacol. 2018. PMID: 29949683
-
Metformin monotherapy for adults with type 2 diabetes mellitus.Cochrane Database Syst Rev. 2020 Jun 5;6(6):CD012906. doi: 10.1002/14651858.CD012906.pub2. Cochrane Database Syst Rev. 2020. PMID: 32501595 Free PMC article.
References
-
- Gupta N, Crouse DL, Miah P, Takaro T. The role of neighbourhood environments in hospitalization risk for diabetes and related conditions: A population-based cohort analysis by remoteness and deprivation indices. Health Rep Dec. 2022;21(12):3–13. 10.25318/82-003-x202201200001. - PubMed
-
- Nagy DK, Bresee LC, Eurich DT, Simpson SH. Are guideline concordant processes of care consistent across the Rural-Urban continuum?? A retrospective cohort study of adults newly treated for type 2 diabetes. Can J Diabetes. 2024;48(5):322–e3295. 10.1016/j.jcjd.2024.03.007. - PubMed
-
- Nagy DK, Bresee LC, Eurich DT, Simpson SH. Rural residence is associated with a delayed trend away from sulfonylurea use for treatment intensification of type 2 diabetes. Diabetes Care Mar. 2023;01(3):613–9. 10.2337/dc22-1223. - PubMed
-
- Booth GL, Hux JE, Fang J, Chan BT. Time trends and geographic disparities in acute complications of diabetes in Ontario, Canada. Diabetes Care May. 2005;28(5):1045–50. 10.2337/diacare.28.5.1045. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
