

Evaluation of the hypercholesterolemia care cascade and compliance with NCEP-ATP III guidelines in Iran based on the WHO STEPS survey
- PMID: 40102862
- PMCID: PMC11921609
- DOI: 10.1186/s12944-025-02506-9
Evaluation of the hypercholesterolemia care cascade and compliance with NCEP-ATP III guidelines in Iran based on the WHO STEPS survey
Abstract
Introduction: Noncommunicable diseases (NCDs), particularly cardiovascular disease (CVD), are the leading cause of death worldwide, with hypercholesterolemia being a major risk factor for CVD. This study evaluated the hypercholesterolemia care cascade in Iran-including prevalence, diagnosis, treatment coverage, and effectiveness-using the National Cholesterol Education Program Adult Treatment Panel III (NCEP-ATP III) guidelines.
Methods: This cross-sectional study drew on data from the 2021 Iran STEPS survey, which employed a systematic cluster sampling of adults aged ≥ 18 years across all provinces in Iran. Hypercholesterolemia was defined per NCEP-ATP III thresholds (LDL ≥ 160 mg/dL, total cholesterol ≥ 240 mg/dL, HDL ≤ 40 mg/dL, or ongoing lipid-lowering therapy). Weighted descriptive statistics were calculated, and Poisson regression with robust variance estimated crude and adjusted prevalence ratios for optimal lipid control among those treated. The 10-year CVD risk was determined using the Framingham Risk Score, stratifying participants into low (< 10%), intermediate (10-20%), and high (> 20%) risk categories.
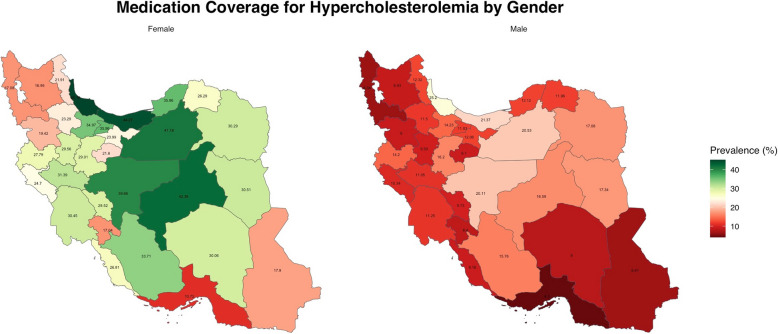
Results: Out of 18,074 participants, 10,582 (55.32%, 95% CI: 54.29-56.35) met NCEP-ATP III criteria for hypercholesterolemia. Among these, only 20.61% (19.55-21.72) were receiving pharmacological treatment. Treatment coverage was notably lower in males (13.15%, 11.98-14.40) than females (29.12%, 27.35-30.96). Statins were the most commonly used medication (11.43% of males, 25.87% of females). Of those receiving treatment, 52.85% (females) and 53.93% (males) achieved optimal LDL, while 76.98% (females) and 81.06% (males) attained total cholesterol < 200 mg/dL. However, only 19.89% (females) and 3.97% (males) met the HDL > 60 mg/dL goal. The 10-year CVD risk was < 10% in 57.79% of participants, 10-20% in 33.27%, and > 20% in 8.94%.
Conclusion: Despite a high prevalence of hypercholesterolemia in Iran, treatment coverage remains suboptimal, particularly among males and working-age adults. Although most treated individuals achieve favorable LDL and total cholesterol levels, gaps persist in achieving optimal HDL targets. These findings underscore the need for strengthened screening, treatment, and adherence strategies-alongside broader preventive measures-to reduce the burden of hypercholesterolemia and CVD in Iran.
Keywords: Cascade of Care; Hypercholesterolemia; Hypolipidemic Agents; Lipid Metabolism Disorders; Risk Reduction Behavior.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The research protocol for the study was approved by the Research Ethics Committees of the Endocrine & Metabolism Research Institute at Tehran University of Medical Sciences, with the approval number IR.TUMS.EMRI.REC.1402.017. Competing interests: The authors declare no competing interests.
Figures

Similar articles
-
Suboptimal control of lipid levels: results from the non-interventional Centralized Pan-Russian Survey of the Undertreatment of Hypercholesterolemia II (CEPHEUS II).Cardiovasc Diabetol. 2017 Dec 16;16(1):158. doi: 10.1186/s12933-017-0641-4. Cardiovasc Diabetol. 2017. PMID: 29246151 Free PMC article.
-
AMG 145, a monoclonal antibody against PCSK9, facilitates achievement of national cholesterol education program-adult treatment panel III low-density lipoprotein cholesterol goals among high-risk patients: an analysis from the LAPLACE-TIMI 57 trial (LDL-C assessment with PCSK9 monoclonal antibody inhibition combined with statin thErapy-thrombolysis in myocardial infarction 57).J Am Coll Cardiol. 2014 Feb 11;63(5):430-3. doi: 10.1016/j.jacc.2013.09.048. Epub 2013 Oct 23. J Am Coll Cardiol. 2014. PMID: 24161333 Clinical Trial.
-
Lipid Screening in Childhood for Detection of Multifactorial Dyslipidemia: A Systematic Evidence Review for the U.S. Preventive Services Task Force [Internet].Rockville (MD): Agency for Healthcare Research and Quality (US); 2016 Aug. Report No.: 14-05204-EF-1. Rockville (MD): Agency for Healthcare Research and Quality (US); 2016 Aug. Report No.: 14-05204-EF-1. PMID: 27559550 Free Books & Documents. Review.
-
Lipid-lowering treatment in hypercholesterolemic patients: the CEPHEUS Thailand survey.J Med Assoc Thai. 2011 Dec;94(12):1424-34. J Med Assoc Thai. 2011. PMID: 22295727
-
Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelines.Circulation. 2004 Jul 13;110(2):227-39. doi: 10.1161/01.CIR.0000133317.49796.0E. Circulation. 2004. PMID: 15249516 Review.
References
-
- UN. Sustainable development goals. 2030. Available at: https://sustainabledevelopment.un.org/?menu513002017.
-
- Aryan Z, Mahmoudi N, Sheidaei A, et al. The prevalence, awareness, and treatment of lipid abnormalities in Iranian adults: Surveillance of risk factors of noncommunicable diseases in Iran 2016. J Clin Lipidol. 2018;12(6):1471-1481.e4. 10.1016/j.jacl.2018.08.001. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
