

Optimizing uni-compartmental knee arthroplasty: the impact of preoperative planning and arithmetic hip-knee-ankle angle
- PMID: 40102874
- PMCID: PMC11916953
- DOI: 10.1186/s12891-025-08512-3
Optimizing uni-compartmental knee arthroplasty: the impact of preoperative planning and arithmetic hip-knee-ankle angle
Abstract
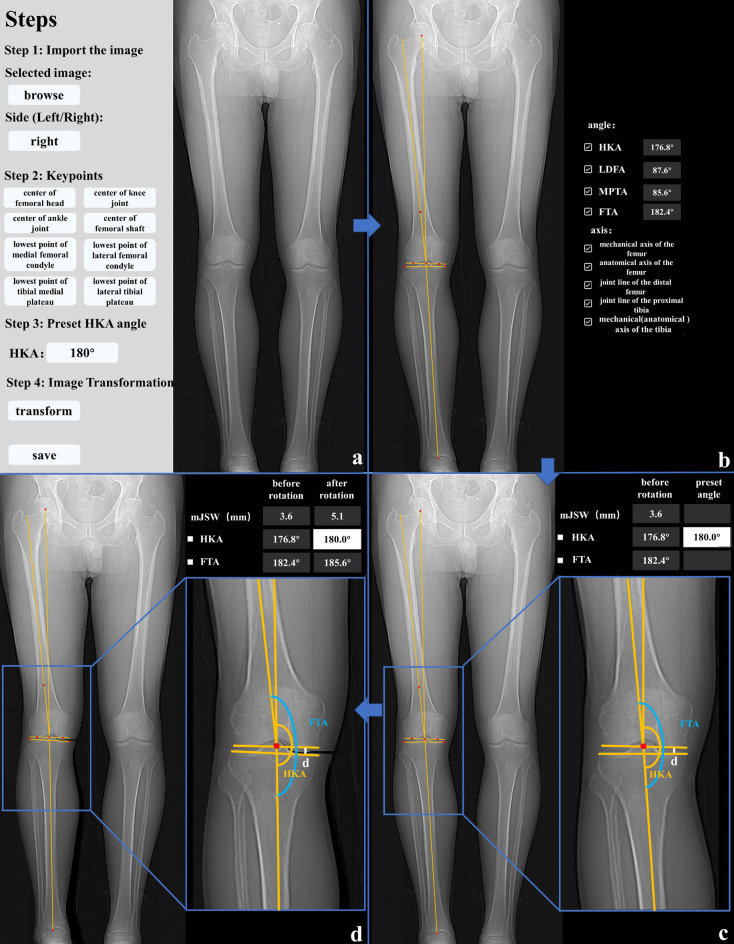
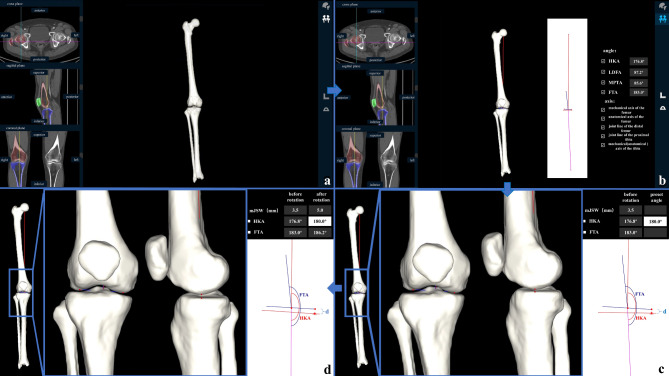
Purpose: The purpose of this study was to evaluate whether the combination of preoperative planning software combined with arithmetic hip-knee-ankle angle (aHKA) can help patients who underwent uni-compartmental knee arthroplasty (UKA) recover the constitutional alignment of the lower limb, obtain a better prosthetic position, and achieve better early patient-reported outcome measurements (PROMs).
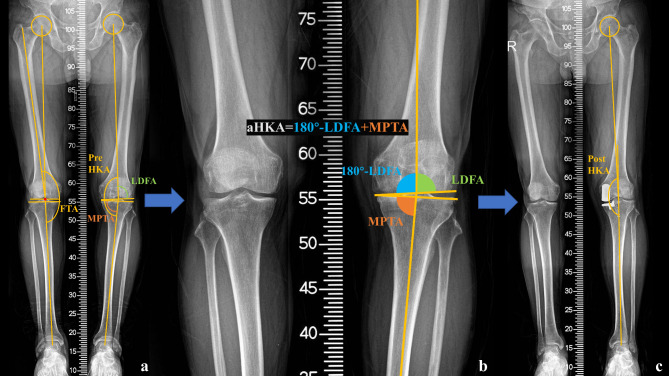
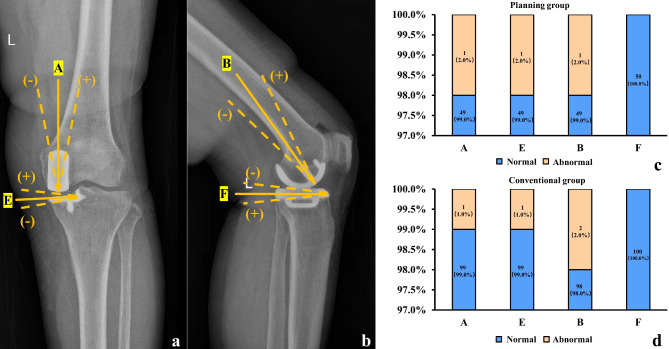
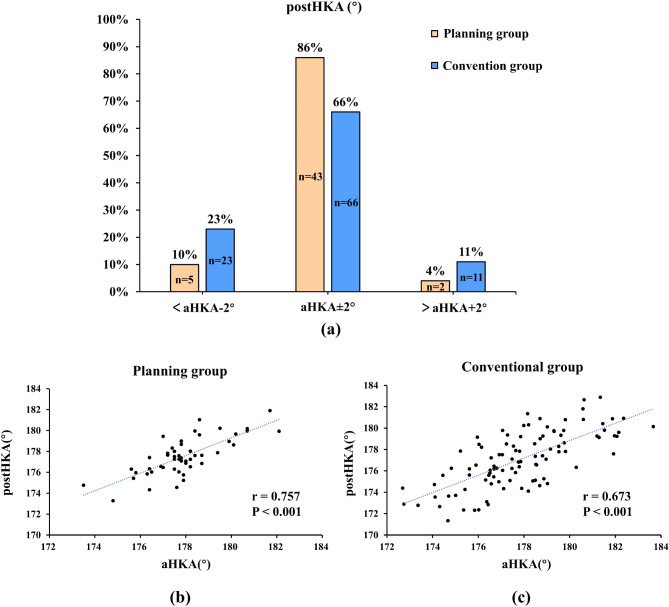
Methods: A total of 150 patients who underwent UKA (planning group: 50 patients using the preoperative planning software; conventional group: 100 patients using the conventional method) were included in the study. The aHKA was defined as 180° + mechanical medial proximal tibial angle (MPTA) - mechanical distal lateral femoral angle (LDFA). All patients in the planning group underwent UKA according to the planning software with the planned lower limb alignment of aHKA. All patients were divided into three groups: constitutional alignment group (postoperative HKA (post-HKA): aHKA ± 2.0°); overcorrection group (post-HKA > aHKA + 2.0°); under-correction group (post-HKA < aHKA - 2.0°). Comparisons between the planning and conventional groups were conducted: (1) the proportion of post-HKA restored to constitutional alignment group; (2) the postoperative prosthesis position parameter based on the guideline of the Oxford group; (3) the American Knee Society scores (KSS) at six months after surgery.
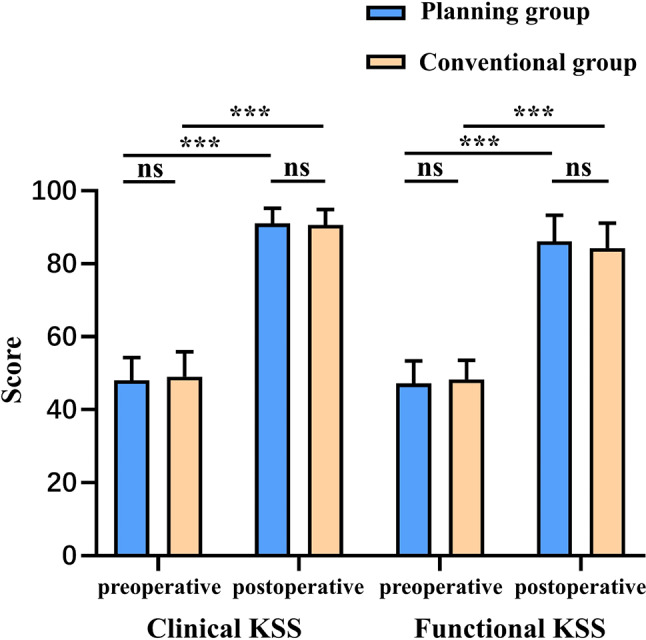
Results: The proportion of the constitutional alignment group in the planning group was higher than that in the conventional group (86% vs. 66%) (p = 0.033). There was no significant difference in postoperative prosthesis position parameters between the two groups. No significant difference was found between the KSS clinical score (91.02 ± 4.20 vs. 90.61 ± 4.24) and KSS functional score (86.10 ± 7.23 vs. 84.30 ± 6.82) in six months after surgery between the planning and conventional groups.
Conclusion: Patients who underwent UKA using preoperative planning software in combination with aHKA were able to recover a higher proportion of the constitutional alignment than those with the conventional method. In addition, the planning group could achieve similar postoperative prosthesis position and short-term PROMs compared to the conventional group.
Clinical trial number: Not applicable.
Keywords: Arithmetic hip-knee-ankle angle (aHKA); Constitutional alignment.; Lower limb alignment; Preoperative planning software; Uni-compartmental knee arthroplasty (UKA).
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the institutional review board of the China-Japan Friendship Hospital (approval number 2020–50-k28). The written informed consent was obtained from all individual participants included in the study. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Slaven SE, Cody JP, Sershon RA, Ho H, Hopper RH Jr., Fricka KB. Alignment in medial Fixed-Bearing unicompartmental knee arthroplasty: the limb has a leg up on the component. J Arthroplasty. 2021;36(12):3883–7. 10.1016/j.arth.2021.08.015. - PubMed
-
- Liu C, Chen H, Ge J, Huang C, Zhang Q, Guo W. Predicting valgus malalignment after mobile-bearing UKA using a new method: the arithmetic HKA of the arthritic knee. Arch Orthop Trauma Surg. 2023;143(10):6381–91. 10.1007/s00402-023-04921-y. - PubMed
-
- Crawford DA, Berend KR, Thienpont E. Unicompartmental knee arthroplasty: US and global perspectives. Orthop Clin North Am. 2020;51(2):147–59. 10.1016/j.ocl.2019.11.010. - PubMed
-
- Grant AL, Doma KD, Hazratwala K. Determination of the accuracy of navigated kinematic unicompartmental knee arthroplasty: A 2-Year Follow-Up. J Arthroplasty. 2017;32(5):1443–52. 10.1016/j.arth.2016.11.036. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
