

The nutritional impact of 7 versus 21 home-delivered medically tailored meals in patients with heart failure and malnutrition risk: a random order crossover feeding trial (MEDIMEALS)
- PMID: 40102963
- PMCID: PMC11916996
- DOI: 10.1186/s40795-025-01036-y
The nutritional impact of 7 versus 21 home-delivered medically tailored meals in patients with heart failure and malnutrition risk: a random order crossover feeding trial (MEDIMEALS)
Abstract
Background: Heart failure (HF) is frequently associated with malnutrition or malnutrition risk. The delivery of medically tailored meals (MTM) to the homes of patients with HF and malnutrition risk or malnutrition after hospital discharge holds promise for improving outcomes. However, the number of MTM needed to provide benefit is not established.
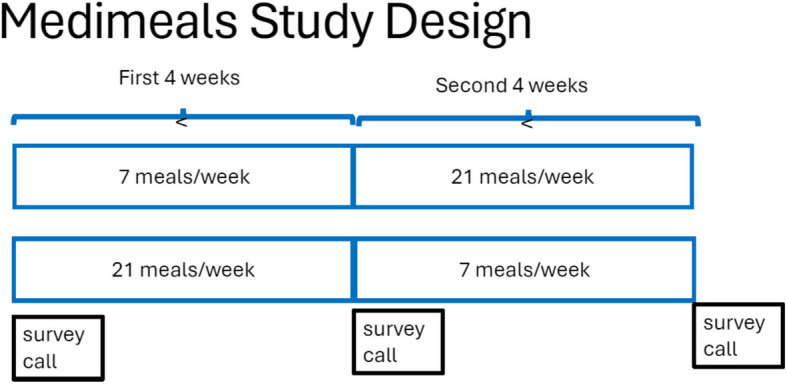
Methods: A random order crossover study was designed to compare the delivery of 7 versus 21 MTM for four weeks each to patients discharged from the hospital with HF and malnutrition risk. Telephone surveys were conducted at baseline, 30, and 60 days post-discharge to evaluate change in malnutrition risk, American Heart Association (AHA) diet goals, sarcopenia risk, and 30-day readmissions.
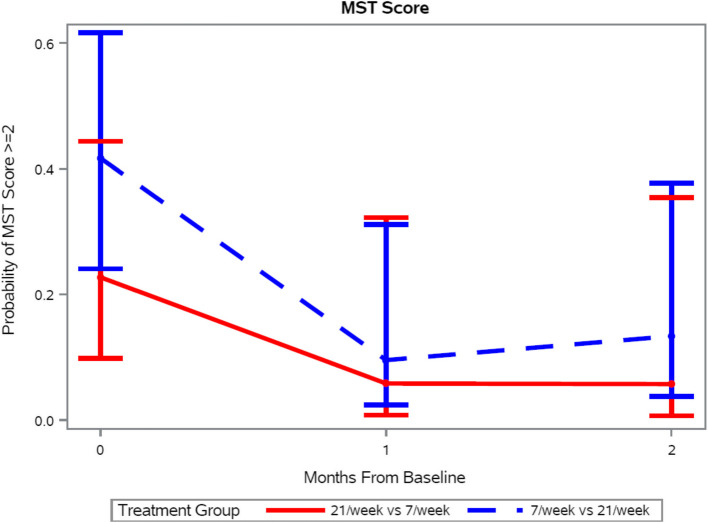
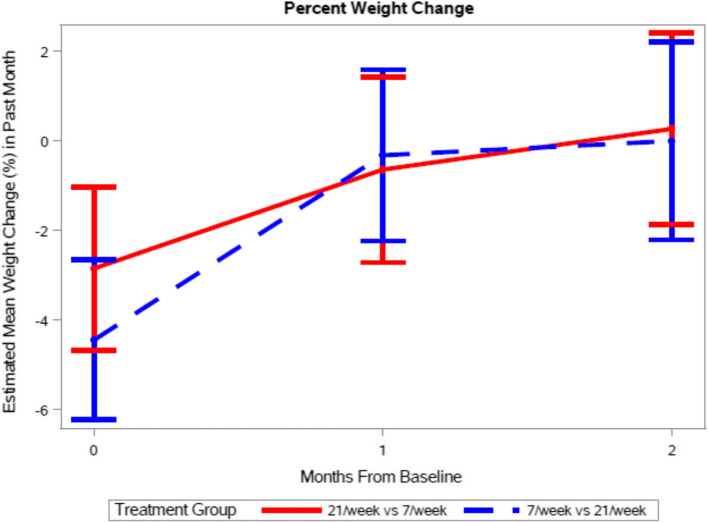
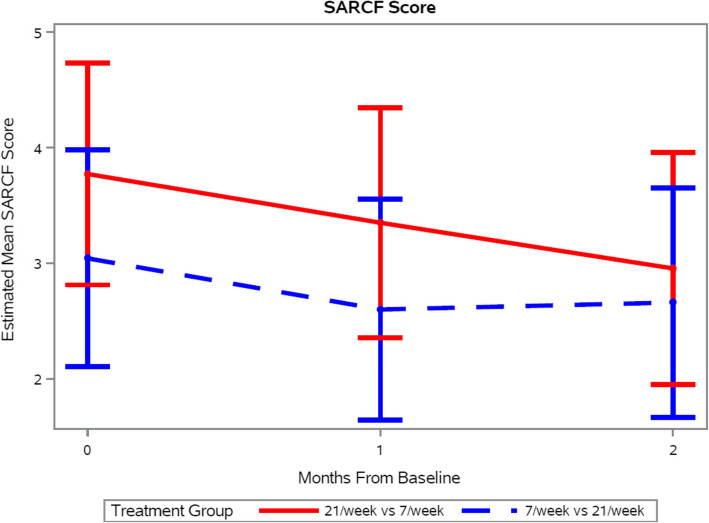
Results: Forty-six patients were enrolled. Patients had reduced odds of having malnutrition risk relative to the baseline score at one and two months (OR 0.18, 95% CI 0.04-0.74 and OR 0.21, 95% CI 0.05-0.99, respectively). The AHA diet score improved over time from baseline by 0.73 ± 0.22 units at one month (p = 0.0014), and by 0.48 ± 0.23 units at two months (p = 0.0430), regardless of the number of MTM provided. Sarcopenia risk improved over time (p = 0.01), decreasing by 0.43 ± 0.2 units by one (p = 0.03) and 0.59 ± 0.21 units by two months (p = 0.007) regardless of the number of MTM provided. Readmissions by 30 days were not significantly different based on the number of MTM provided (9% for 21 MTM vs 12.5% for 7 MTM), but well below national data at 23%.
Conclusion: The provision of at least seven MTM per week in the early window after hospital discharge to patients with HF and malnutrition or malnutrition risk is a promising strategy to improve malnutrition and sarcopenia risk and diet adherence, while keeping readmissions below national averages.
Trial registration: Clinicaltrials.gov NCT06142903, registered 11/23/2023.
Keywords: Heart failure; MST; Malnutrition risk; Medically tailored meals; SARC-F.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participte: Ethics approval was obtained from the University of Pennsylvania Institutional Review Board number 1 protocol number 814914, and all patients gave informed consent using an approved consent document. The study was conducted in compliance with the Declaration of Helsinki. Consent for publication: N/a. Competing interests: The authors declare no competing interests.
Figures

References
-
- WS C. Overview of the management of heart failure with reduced ejection fraction in adults: UpToDate; 2024 [updated 03/04/2024. Available from: https://pennmedaccess.uphs.upenn.edu/f5-w-68747470733a2f2f7777772e757074....
-
- Prevention CfDCa. Heart Disease Facts 2021 [cited 2021 10/17]. Available from: https://www.cdc.gov/heartdisease/facts.htm.
-
- Jensen GL, Cederholm T, Correia M, Gonzalez MC, Fukushima R, Higashiguchi T, et al. GLIM Criteria for the Diagnosis of Malnutrition: A Consensus Report From the Global Clinical Nutrition Community. JPEN J Parenter Enteral Nutr. 2019;43(1):32–40. - PubMed
-
- Jensen GL, Cederholm T, Ballesteros-Pomar MD, Blaauw R, Correia M, Cuerda C, et al. Guidance for assessment of the inflammation etiologic criterion for the GLIM diagnosis of malnutrition: A modified Delphi approach. JPEN J Parenter Enteral Nutr. 2024;48(2):145–54. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous