

Management of delayed corneal epithelial healing after refractive surgery: five case reports
- PMID: 40103788
- PMCID: PMC11913852
- DOI: 10.3389/fmed.2025.1517403
Management of delayed corneal epithelial healing after refractive surgery: five case reports
Abstract
Background: Transepithelial photorefractive keratectomy using Smart Pulse Technology (SPT-TransPRK) is currently the leading method for superficial refractive surgery, offering advantages such as a non-contact procedure, shorter operation times, and excellent patient cooperation. Laser ablation of the corneal epithelium, Bowman's membrane, and the stroma can effectively correct refractive errors. Thus, the complete healing of the corneal epithelium post-surgery is essential for ensuring good vision. Refractive surgeons should enhance their understanding of corneal wound healing mechanisms and focus on the repair of the corneal epithelium following refractive surgery to ensure the quality of visual health of patients.
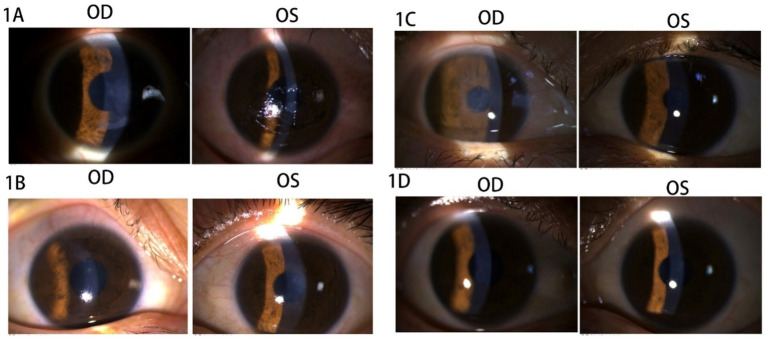
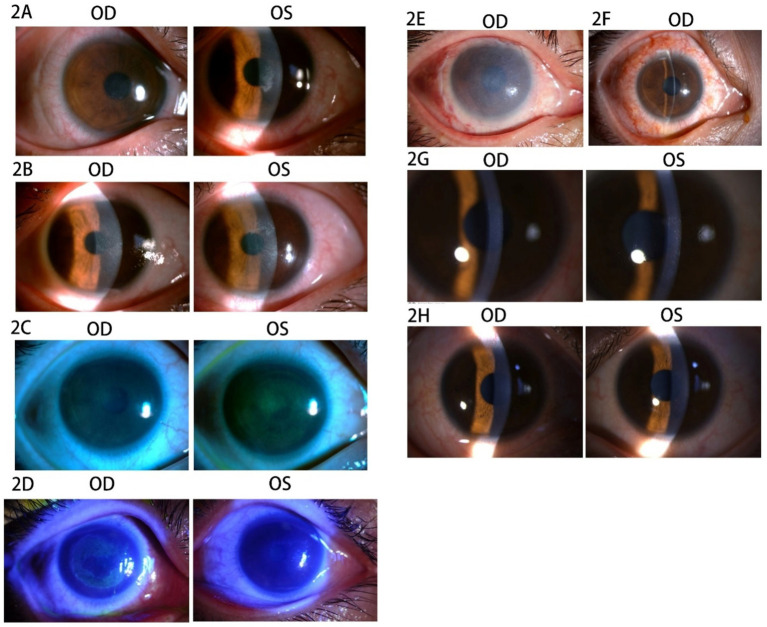
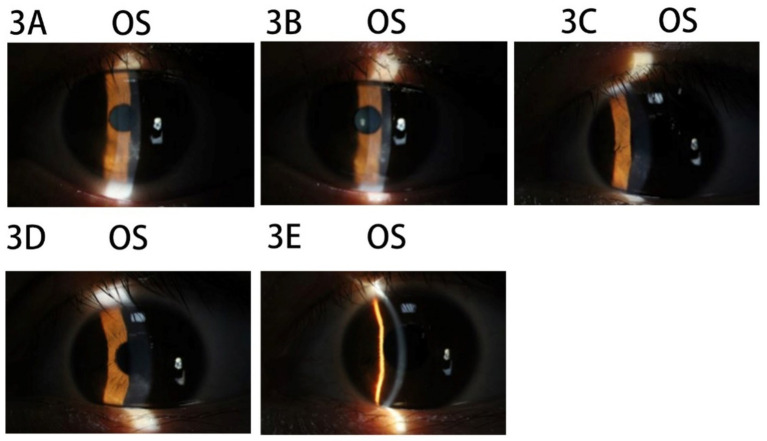
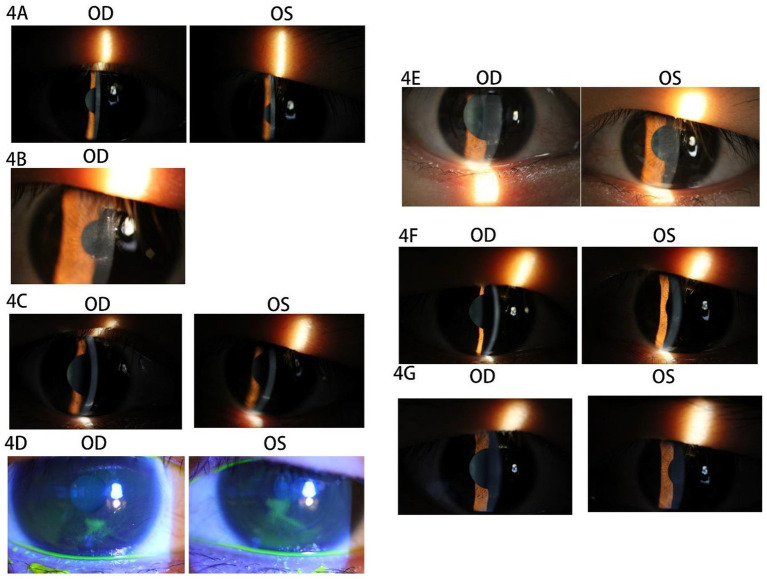
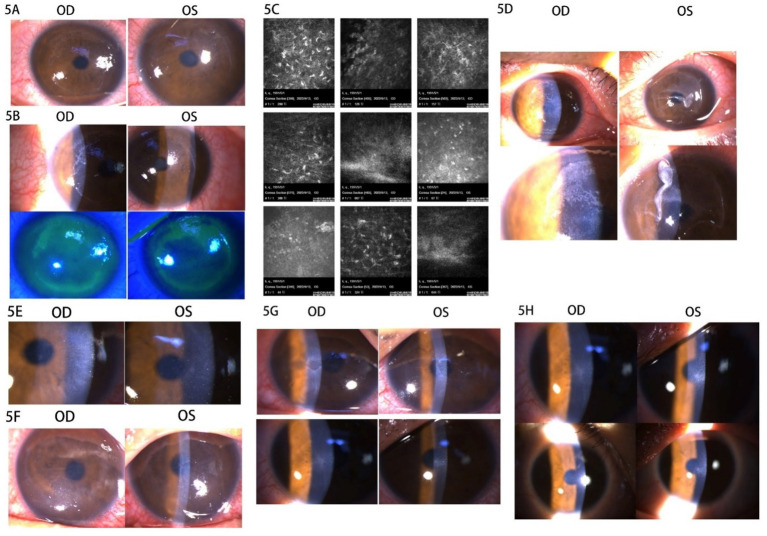
Case presentation: A total of five patients experienced varying degrees of delayed corneal epithelial healing following refractive surgery. In Case 1, unhealthy corneal epithelial debris was removed, and ophthalmic ointment was applied to cover the eyes instead of using bandage contact lenses (BCLs) to reconstruct the corneal epithelial barrier. This approach was also successfully implemented in Case 2. Furthermore, amniotic membrane transplantation (AMT) can quickly establish a corneal barrier and promote corneal epithelial regeneration, especially in cases of extensive corneal epithelial detachment. The remaining three patients were suspected of having corneal viral infections based on their medical history and the observation of corneal pathology using a slit lamp microscope. To prevent further infection and promote regeneration, topical steroid drops were discontinued early, and topical antiviral and corneal epithelial regeneration medications were administered alongside systemic antiviral therapy. Steroid drops were resumed after corneal epithelial healing to effectively prevent post-refractive haze.
Conclusion: Delays in corneal epithelial healing after refractive surgery should be taken seriously. BCLs, steroids, and both topical and systemic antiviral therapies should be properly utilized when there is a delay in corneal epithelial healing.
Keywords: corneal virus infection; delayed corneal epithelial healing; persistent epithelial defects; refractive surgery; trans-PRK.
Copyright © 2025 Yan, Jin, Zhang, Liu, Yu, Zhao, Mu, Xu and Zhang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
[Confocal microscopy of the corneal after photorefractive keratectomy with the excimer laser].Klin Monbl Augenheilkd. 1997 Sep;211(3):159-67. doi: 10.1055/s-2008-1035116. Klin Monbl Augenheilkd. 1997. PMID: 9445896 German.
-
Stromal wound healing explains refractive instability and haze development after photorefractive keratectomy: a 1-year confocal microscopic study.Ophthalmology. 2000 Jul;107(7):1235-45. doi: 10.1016/s0161-6420(00)00142-1. Ophthalmology. 2000. PMID: 10889092
-
Collagen cross-linking using riboflavin and ultraviolet-a for corneal thinning disorders: an evidence-based analysis.Ont Health Technol Assess Ser. 2011;11(5):1-89. Epub 2011 Nov 1. Ont Health Technol Assess Ser. 2011. PMID: 23074417 Free PMC article.
-
Corneal Regeneration After Photorefractive Keratectomy: A Review.J Optom. 2015 Jul-Sep;8(3):149-69. doi: 10.1016/j.optom.2014.09.001. Epub 2014 Oct 23. J Optom. 2015. PMID: 25444646 Free PMC article. Review.
-
Transepithelial Photorefractive Keratectomy-Review.Vision (Basel). 2024 Mar 21;8(1):16. doi: 10.3390/vision8010016. Vision (Basel). 2024. PMID: 38535765 Free PMC article. Review.
References
-
- Alkadi T, Alanazi S, Algwaiz A, Alyahya S, Binyousef F. Early visual and clinical outcomes of transepithelial photorefractive keratectomy versus transepithelial keratectomy with smart pulse technology for myopia. Oman J Ophthalmol. (2024) 17:337–41. doi: 10.4103/ojo.ojo_212_23, PMID: - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources