

Haemodynamic spectrum in heritable pulmonary arterial hypertension: a continuum from pre-capillary to combined pulmonary hypertension-case series
- PMID: 40103798
- PMCID: PMC11913607
- DOI: 10.1093/ehjcr/ytaf109
Haemodynamic spectrum in heritable pulmonary arterial hypertension: a continuum from pre-capillary to combined pulmonary hypertension-case series
Abstract
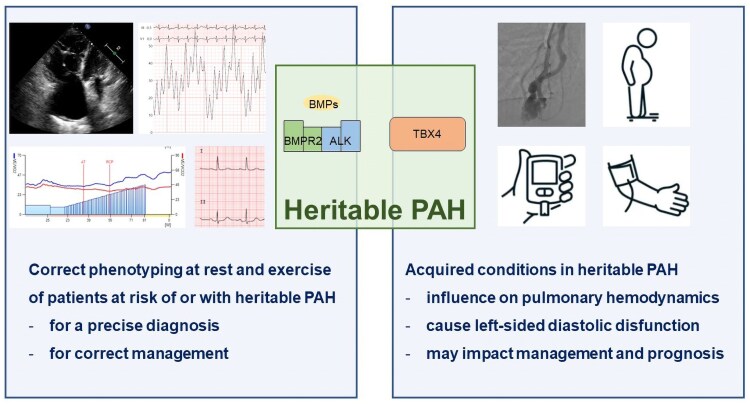
Background: Heritable pulmonary arterial hypertension (PAH) is a rare form of pre-capillary pulmonary hypertension that typically affects young patients. With increased survival and subsequent ageing of these patients, newly acquired cardiovascular conditions may influence the pulmonary haemodynamic profile and impact management.
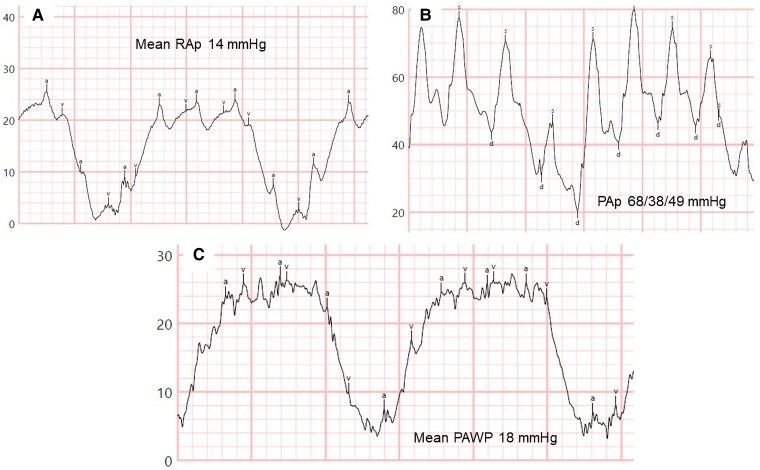
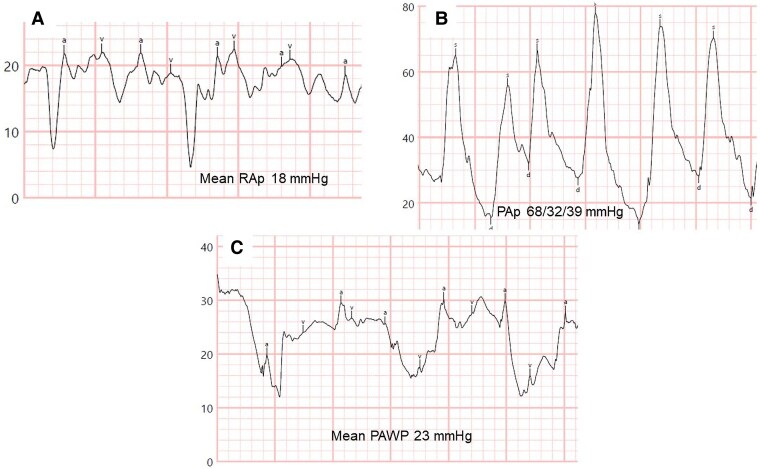
Case summary: We report a case series of four patients with mutations in genes associated with PAH to illustrate the spectrum of pulmonary haemodynamics under the influence of superimposed acquired conditions. The first two cases involve patients with a long-standing diagnosis of heritable PAH and severe pre-capillary pulmonary hypertension, who developed overt left-sided diastolic dysfunction later in follow-up due to the acquisition of multiple cardiovascular comorbidities. The second two cases describe patients with a genetic pre-disposition to develop PAH and conditions that are risk factors for left heart disease, with mild elevation of resting pulmonary pressures, in whom exercise right heart catheterization unmasked occult left-sided diastolic dysfunction.
Discussion: Pulmonary haemodynamics are complex and dynamic over time, even in patients with or at risk of heritable PAH, when additional acquired cardiovascular conditions emerge. Correct phenotyping at diagnosis and during follow-up of patients at risk of heritable PAH, along with a clear understanding of the underlying pulmonary haemodynamic profile, is crucial for appropriate management.
Keywords: Cardiovascular comorbidities; Case series; Diastolic dysfunction; Exercise right heart catheterization; Heritable pulmonary arterial hypertension; Post-capillary pulmonary hypertension; Pre-capillary pulmonary hypertension.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest. None declared.
Figures
Similar articles
-
Clinical phenotypes and outcomes of pulmonary hypertension due to left heart disease: Role of the pre-capillary component.PLoS One. 2018 Jun 19;13(6):e0199164. doi: 10.1371/journal.pone.0199164. eCollection 2018. PLoS One. 2018. PMID: 29920539 Free PMC article.
-
Clinical and Biological Insights Into Combined Post- and Pre-Capillary Pulmonary Hypertension.J Am Coll Cardiol. 2016 Dec 13;68(23):2525-2536. doi: 10.1016/j.jacc.2016.09.942. J Am Coll Cardiol. 2016. PMID: 27931609 Free PMC article.
-
Prevalence and prognostic value of left ventricular diastolic dysfunction in idiopathic and heritable pulmonary arterial hypertension.Chest. 2012 Jun;141(6):1457-1465. doi: 10.1378/chest.11-1903. Epub 2011 Dec 29. Chest. 2012. PMID: 22207680 Free PMC article.
-
Role of Exercise Stress Echocardiography in Pulmonary Hypertension.Life (Basel). 2023 Jun 14;13(6):1385. doi: 10.3390/life13061385. Life (Basel). 2023. PMID: 37374168 Free PMC article. Review.
-
Pulmonary arterial hypertension.Orphanet J Rare Dis. 2013 Jul 6;8:97. doi: 10.1186/1750-1172-8-97. Orphanet J Rare Dis. 2013. PMID: 23829793 Free PMC article. Review.
References
-
- Hassoun PM. Pulmonary arterial hypertension. N Engl J Med 2021;385:2361–2376. - PubMed
-
- Humbert M, Kovacs G, Hoeper MM, Badagliacca R, Berger RMF, Brida M, et al. 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension: developed by the task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS). Endorsed by the International Society for heart and lung transplantation (ISHLT) and the European reference network on rare respiratory diseases (ERN-LUNG). Eur Heart J 2022;43:3618–3731. - PubMed
-
- Sztrymf B, Coulet F, Girerd B, Yaici A, Jais X, Sitbon O, et al. Clinical outcomes of pulmonary arterial hypertension in carriers of BMPR2 mutation. Am J Respir Crit Care Med 2008;177:1377–1383. - PubMed
Publication types
LinkOut - more resources
Full Text Sources