

The current state of cranioplasty in Europe - Results from a European cranioplasty survey
- PMID: 40103849
- PMCID: PMC11914825
- DOI: 10.1016/j.bas.2025.104214
The current state of cranioplasty in Europe - Results from a European cranioplasty survey
Abstract
Introduction: Cranioplasty, a surgical procedure to restore skull integrity and aesthetic contour following decompressive craniectomy, poses challenges in material selection and timing, driven by the lack of guidelines and ongoing regulatory changes.
Research question: This study aimed to provide an overview of current cranioplasty practices in Europe, explicitly addressing a potential shift towards alloplastic materials and the management of patients with concomitant hydrocephalus.
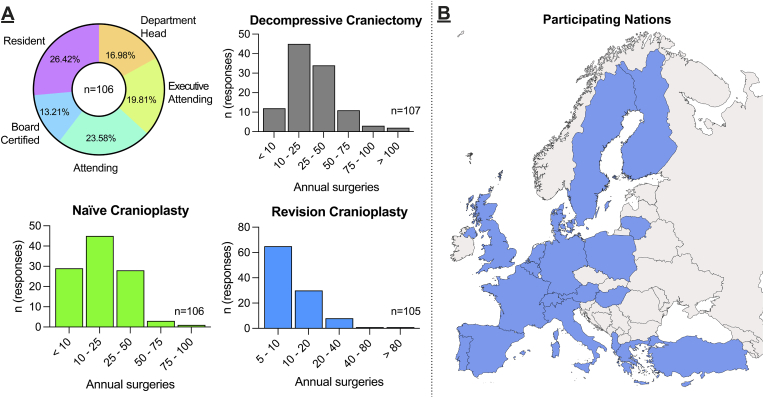
Material and methods: An online survey was conducted among European neurosurgical centers from January to March 2024, collecting data on material preferences, timing of procedures, and management strategies for cranioplasty. Descriptive and statistical analyses were performed on 110 complete responses.
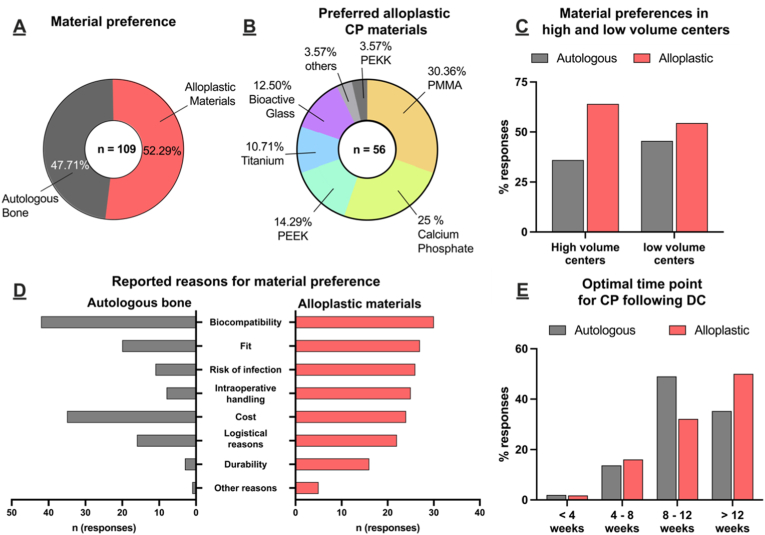
Results: Respondents favored alloplastic materials over autologous bone for cranioplasty, citing regulatory constraints and reduced infection risk as primary reasons. Variability was observed in the timing of procedures and the management of patients with hydrocephalus, with most centers adopting staged approaches.
Discussion and conclusion: The shift towards alloplastic materials in cranioplasty reflects regulatory pressures rather than material-specific considerations. Despite variability in practice, our findings underscore the need for standardized guidelines and further research to optimize patient outcomes. This study provides valuable insights into current practices and highlights areas for future investigation in cranioplasty.
Keywords: Alloplastic materials; Autologous bone; Cranioplasty; European survey; Hydrocephalus management; Regulatory changes.
© 2025 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

References
-
- Chan D.Y.C., Mok Y.T., Lam P.K., Tong C.S.W., Ng S.C.P., Sun T.F.D., Poon W.S. Cryostored autologous skull bone for cranioplasty? A study on cranial bone flaps' viability and microbial contamination after deep-frozen storage at −80 °C. J. Clin. Neurosci. 2017;42:81–83. doi: 10.1016/j.jocn.2017.04.016. - DOI - PubMed
LinkOut - more resources
Full Text Sources
