

Intra-abdominal Mucormycosis in an Immunocompetent Host: A Rare Presentation and Literature Review
- PMID: 40103914
- PMCID: PMC11913594
- DOI: 10.7759/cureus.80730
Intra-abdominal Mucormycosis in an Immunocompetent Host: A Rare Presentation and Literature Review
Abstract
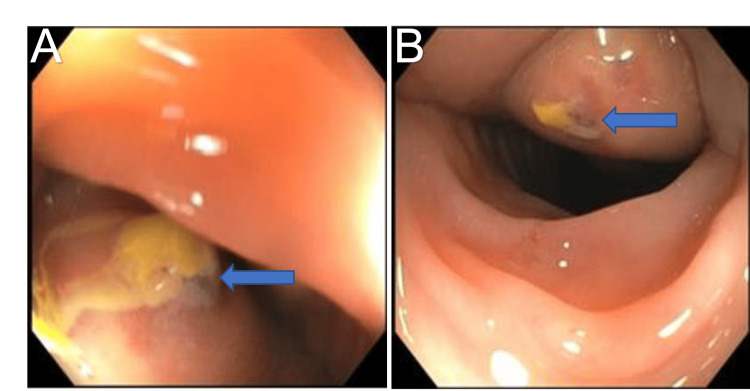
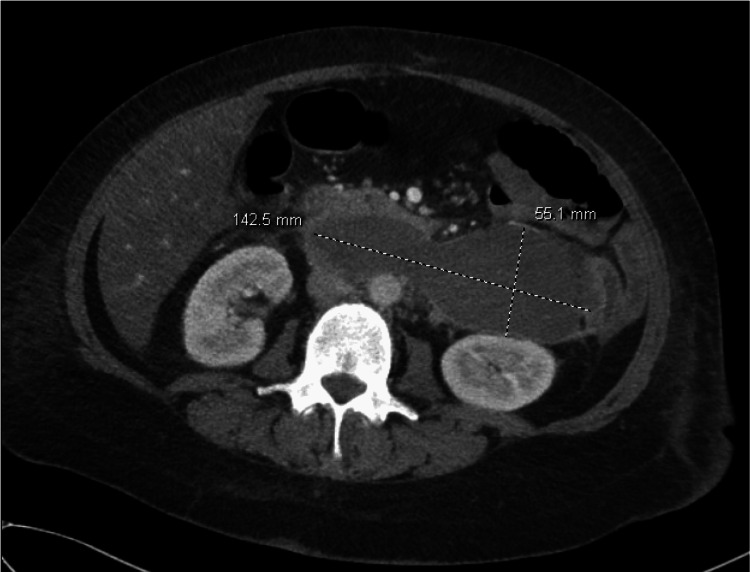
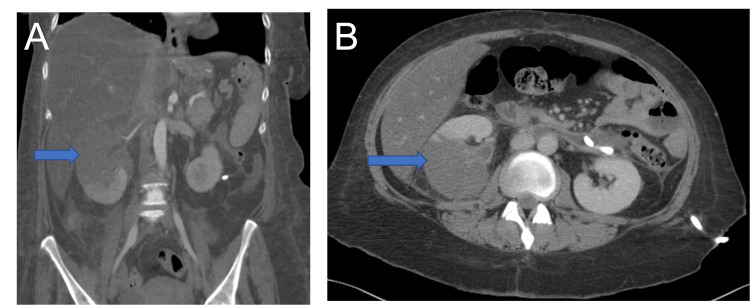
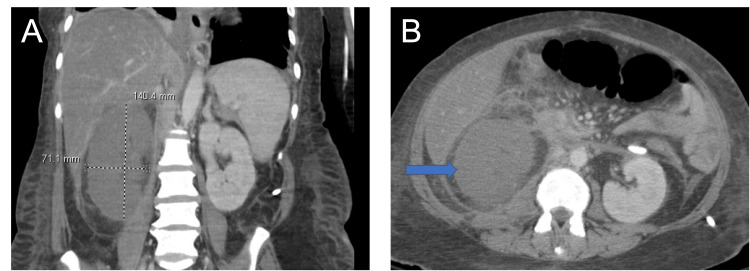
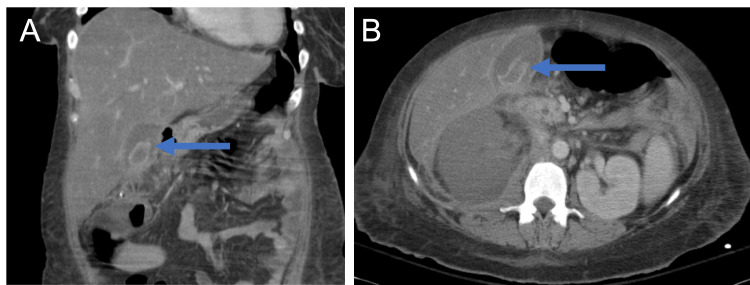
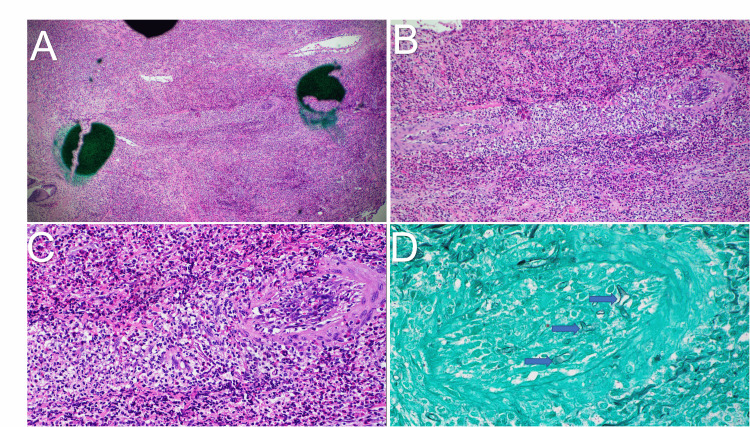
Mucormycosis is a severe, opportunistic infection caused by Mucorales, a taxonomical group of thermotolerant fungi primarily affecting the immunocompromised. Intra-abdominal involvement in mucormycosis is a rare entity, particularly in immunocompetent individuals. We present a fatal case of gallbladder and renal mucormycosis in an immunocompetent female, leading to septic shock and death. The diagnosis was confirmed via histopathology following cholecystectomy for suspected gangrenous cholecystitis and open right nephrectomy due to kidney infarction. Quantitative polymerase chain reaction of the tissue identified the presence of Apophysomyces ossiformis. The clinical picture was confounded by ongoing sepsis due to a Klebsiella pneumoniae-infected retroperitoneal hematoma, non-specific imaging findings, and the absence of traditional risk factors for mucormycosis, leading to a delayed diagnosis. Despite surgical debridement, initiation of liposomal amphotericin B with posaconazole, and aggressive treatment in the intensive care unit, the patient succumbed to complications of mucormycosis. Despite adequate antibiotic coverage, this case underscores the importance of considering Mucorales infection in otherwise immunocompetent patients with a deteriorating clinical condition. Early diagnosis and appropriate intervention are essential in enhancing mucormycosis survivability, though mortality rates remain high in severe cases.
Keywords: apophysomyces ossiformis; diagnostic challenges; gallbladder mucormycosis; liposomal amphotericin b; renal mucormycosis; septic shock.
Copyright © 2025, Hamamah et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Rhino-orbital mucormycosis due to Apophysomyces ossiformis in a patient with diabetes mellitus: a case report.BMC Infect Dis. 2020 Aug 18;20(1):614. doi: 10.1186/s12879-020-05337-4. BMC Infect Dis. 2020. PMID: 32811466 Free PMC article.
-
Mucormycosis Caused by Apophysomyces elegans-A Case Report and Systematic Review of the Literature of Rhino-Orbito-Cerebral Cases of the Genus Apophysomyces.J Fungi (Basel). 2025 May 9;11(5):368. doi: 10.3390/jof11050368. J Fungi (Basel). 2025. PMID: 40422702 Free PMC article. Review.
-
Survival after rhino-orbital-cerebral mucormycosis in an immunocompetent patient.Ophthalmology. 2000 Mar;107(3):555-8. doi: 10.1016/s0161-6420(99)00142-6. Ophthalmology. 2000. PMID: 10711895
-
Chronical rhino-orbital mucormycosis in an immunocompetent host: A case report.Int J Surg Case Rep. 2021 May;82:105882. doi: 10.1016/j.ijscr.2021.105882. Epub 2021 Apr 10. Int J Surg Case Rep. 2021. PMID: 33865198 Free PMC article.
-
Our 2014 approach to mucormycosis.Mycoses. 2014 Sep;57(9):519-24. doi: 10.1111/myc.12203. Epub 2014 May 15. Mycoses. 2014. PMID: 24829170 Review.
References
-
- Mucormycosis. Czech MM, Cuellar-Rodriguez J. https://www.sciencedirect.com/science/article/abs/pii/S0891552024000837?.... Infect Dis Clin North Am. 2025;39:121–144. - PMC - PubMed
-
- Part 1: mucormycosis: prevalence, risk factors, clinical features, and diagnosis. Lynch JP 3rd, Fishbein MC, Abtin F, Zhanel GG. Expert Rev Anti Infect Ther. 2023;21:723–736. - PubMed
-
- Hernández JL, Buckley CJ. Treasure Island, FL: StatPearls Publishing; Mucormycosis. - PubMed
-
- The epidemiology and clinical manifestations of mucormycosis: a systematic review and meta-analysis of case reports. Jeong W, Keighley C, Wolfe R, Lee WL, Slavin MA, Kong DC, Chen SC. Clin Microbiol Infect. 2019;25:26–34. - PubMed
Publication types
LinkOut - more resources
Full Text Sources