

Providing continuity of care for people living with noncommunicable diseases in humanitarian settings: A qualitative study of health actors' experiences in Lebanon
- PMID: 40103922
- PMCID: PMC11915524
- DOI: 10.1016/j.jmh.2024.100269
Providing continuity of care for people living with noncommunicable diseases in humanitarian settings: A qualitative study of health actors' experiences in Lebanon
Abstract
Objective: The burden of non-communicable diseases (NCDs) is increasing among populations living in humanitarian settings. Continuity of care (CoC) involves following an individual over time and across different levels of healthcare (management, longitudinal, informational and interpersonal continuity); it is an essential component of good quality, person-centred NCD care. Providing CoC is particularly challenging in humanitarian crises where health care access may be interrupted or restricted. This paper aimed to explore health actors' experiences of continuity of hypertension and diabetes care for Syrian refugees and vulnerable Lebanese in Lebanon.
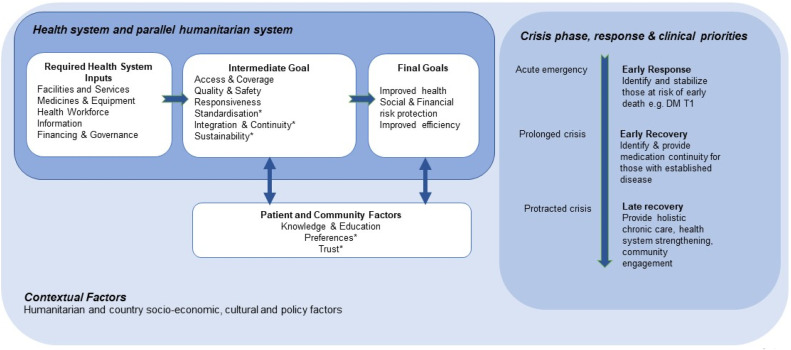
Methods: We conducted 20 in-depth qualitative interviews with health actors, including eleven with health care providers at four urban-based health facilities supported by international humanitarian agencies that provide NCD care to Syrian refugees and vulnerable Lebanese, one representative of a governmental institution, one international delegate and seven humanitarian actors. Thematic analysis, combining inductive and deductive approaches, was guided by a conceptual framework for NCD models of care in humanitarian settings. We reported our findings against the conceptual framework's domains relating to health system inputs and intermediate goals, reflecting on their impact on the domains of CoC.
Findings: Existing health system weaknesses and novel challenges (the economic crisis, COVID-19 pandemic and Beirut blast) to continuity of NCD care were identified. Health system input challenges: governance and financing (weakened governance, limited central financing, historical dependence on local NGOs for primary healthcare, a dominant private sector), health workforce (exodus of health care providers from the public system), inconsistent medicines and equipment supplies, and limited health information systems (no unified system across institutions or levels of care, lack of formal referral systems, and inconsistent facility-level data collection) contributed to limited public primary care, poorly integrated within a fragile, pluralistic health system. These factors negatively impacted the intermediate health system goals of access, standardisation and quality of NCD care for Syrian refugee and Lebanese patients, and collectively hampered the management, longitudinal, informational and interpersonal continuity of NCD care in Lebanon.
Conclusion: We recommend that humanitarian actors continue the work underway with the Lebanese Ministry of Public Health to align with and strengthen health system inputs, including supporting health governance through the accreditation process, exploring new funding mechanisms, strengthening the workforce via task sharing and training, supporting the medication supply chain, improving access to facilities and service quality, and supporting the development, standardisation and interoperability of referral and information systems. In combination, these elements will support better CoC for people living with hypertension and diabetes in Lebanon.
Keywords: Conflict; Continuity of care; Health service; Humanitarian; Integration; Noncommunicable disease; Person centred.
© 2024 The Authors. Published by Elsevier Ltd.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Decentralising healthcare for diabetes and hypertension from secondary to primary level in a humanitarian setting in Kurdistan, Iraq: a qualitative study.BMC Health Serv Res. 2025 Apr 15;25(1):548. doi: 10.1186/s12913-025-12571-6. BMC Health Serv Res. 2025. PMID: 40234891 Free PMC article.
-
Chronic NCD care in crises: A qualitative study of global experts' perspectives on models of care for hypertension and diabetes in humanitarian settings.J Migr Health. 2022 Mar 24;5:100094. doi: 10.1016/j.jmh.2022.100094. eCollection 2022. J Migr Health. 2022. PMID: 35434681 Free PMC article.
-
Lessons from the COVID-19 pandemic to strengthen NCD care and policy in humanitarian settings: a mixed methods study exploring humanitarian actors' experiences.BMC Health Serv Res. 2024 Sep 17;24(1):1081. doi: 10.1186/s12913-024-11458-2. BMC Health Serv Res. 2024. PMID: 39289744 Free PMC article.
-
Host country responses to non-communicable diseases amongst Syrian refugees: a review.Confl Health. 2019 Mar 22;13:8. doi: 10.1186/s13031-019-0192-2. eCollection 2019. Confl Health. 2019. PMID: 30949232 Free PMC article. Review.
-
Models of care for patients with hypertension and diabetes in humanitarian crises: a systematic review.Health Policy Plan. 2021 May 17;36(4):509-532. doi: 10.1093/heapol/czab007. Health Policy Plan. 2021. PMID: 33693657 Free PMC article.
Cited by
-
Decentralising healthcare for diabetes and hypertension from secondary to primary level in a humanitarian setting in Kurdistan, Iraq: a qualitative study.BMC Health Serv Res. 2025 Apr 15;25(1):548. doi: 10.1186/s12913-025-12571-6. BMC Health Serv Res. 2025. PMID: 40234891 Free PMC article.
-
Breast and Cervical Cancer Gaps in Displaced Lebanese Women in Syria.JAMA Netw Open. 2025 Aug 1;8(8):e2525652. doi: 10.1001/jamanetworkopen.2025.25652. JAMA Netw Open. 2025. PMID: 40768145 Free PMC article.
References
-
- Agency for Healthcare Research and Quality. Care coordination. Content last reviewed August 2018. 2018 [Available from: https://www.ahrq.gov/ncepcr/care/coordination.html.
-
- American Academy of Family Physicians. 2024 Continuity of care, definition of 2023 [Available from: https://www.aafp.org/about/policies/all/continuity-of-care-definition.html.
-
- Ansbro É., Homan T., Qasem J., Bil K., Rasoul Tarawneh M., Roberts B., et al. MSF experiences of providing multidisciplinary primary level NCD care for Syrian refugees and the host population in Jordan: an implementation study guided by the RE-AIM framework. BMC Health Serv. Res. 2021;21:1–19. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
