

Divergent responses to SARS-CoV-2 infection in bronchial epithelium with pre-existing respiratory diseases
- PMID: 40104058
- PMCID: PMC11914195
- DOI: 10.1016/j.isci.2025.111999
Divergent responses to SARS-CoV-2 infection in bronchial epithelium with pre-existing respiratory diseases
Abstract
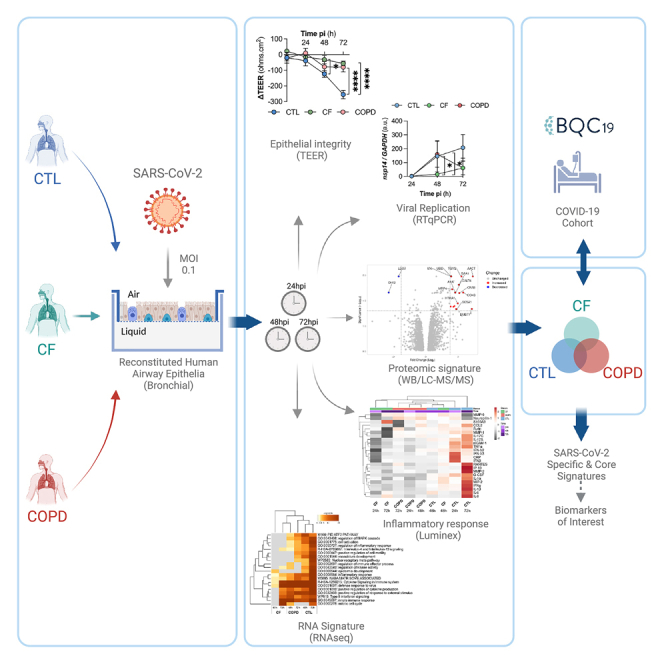
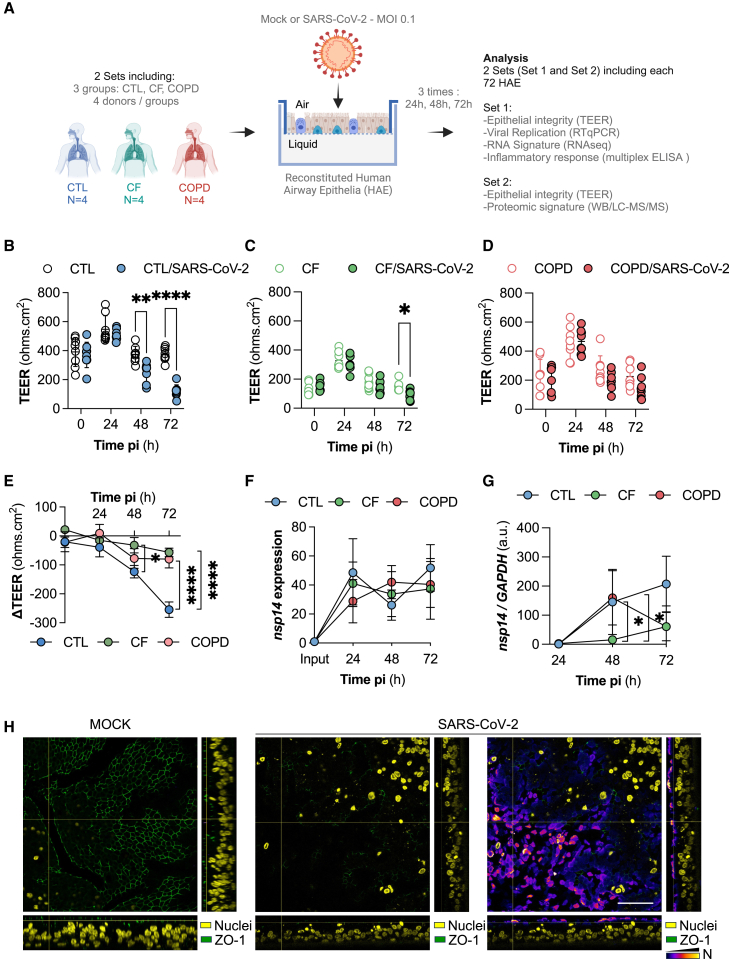
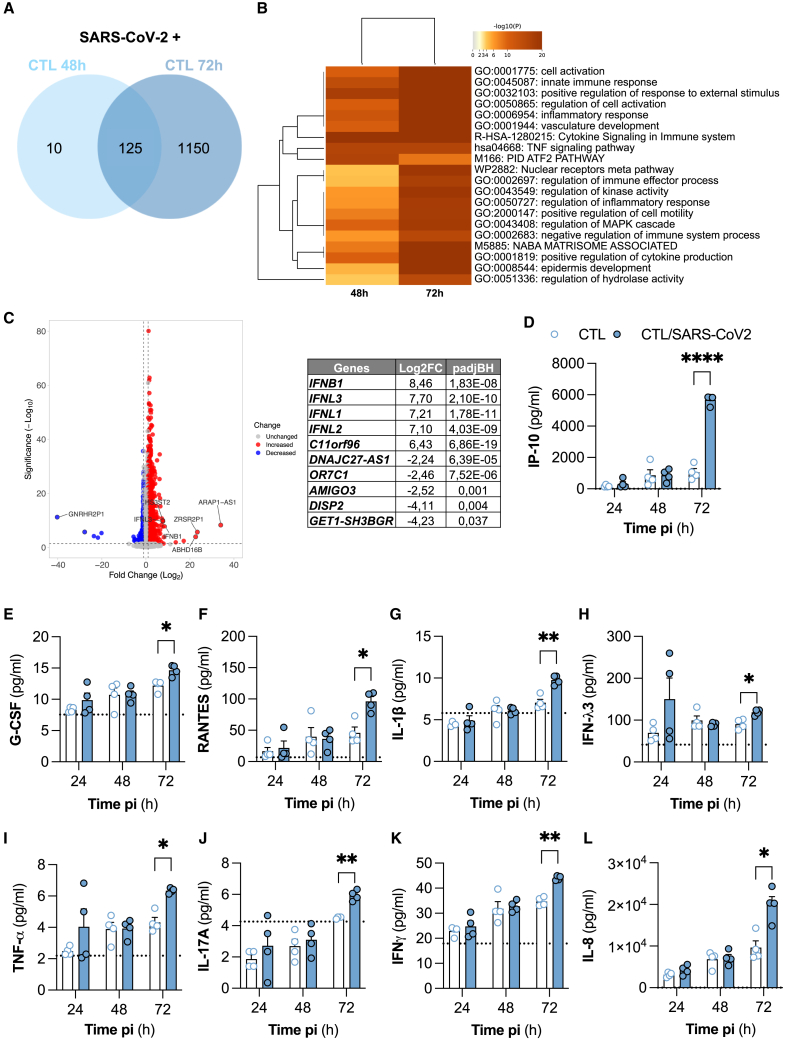
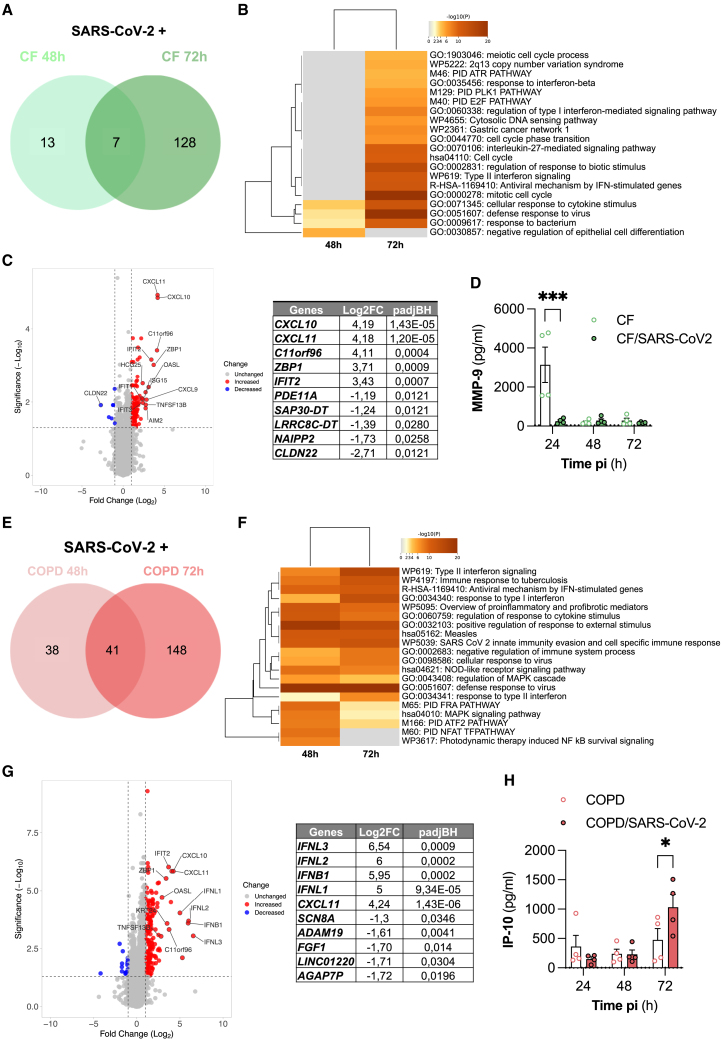
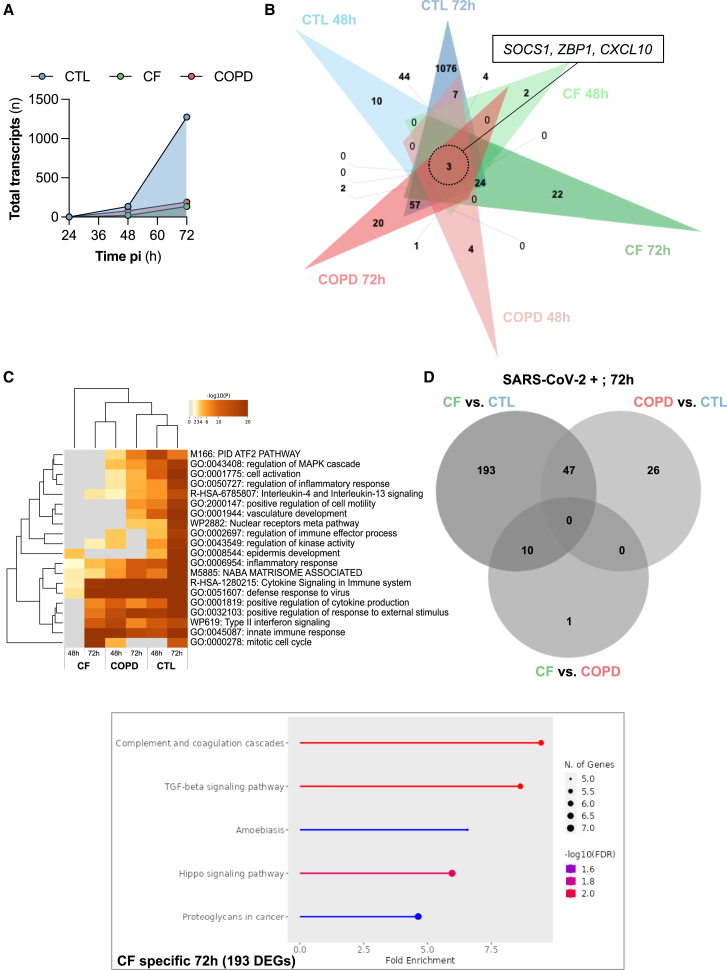
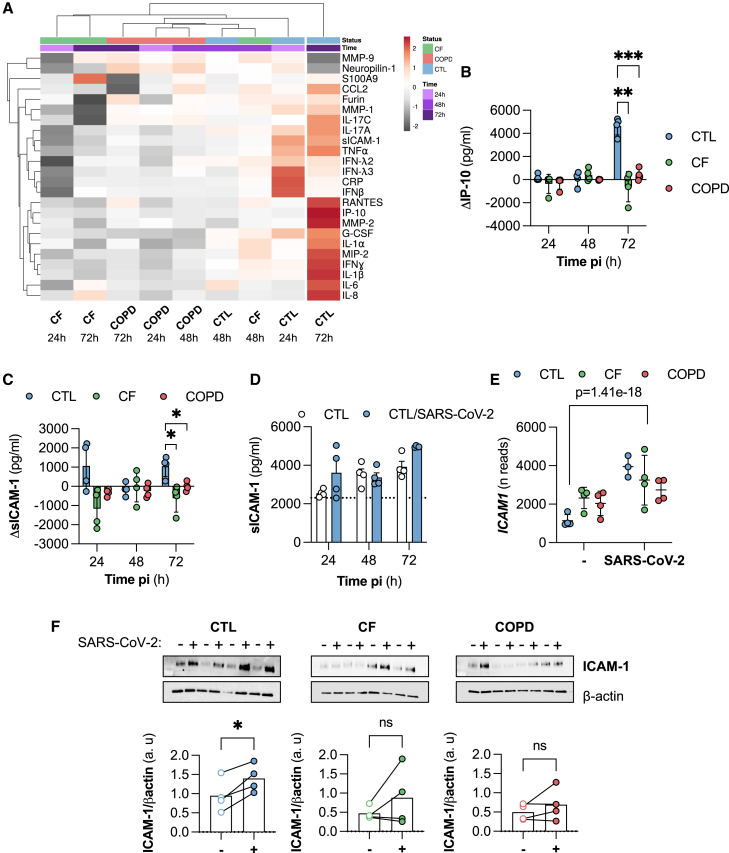
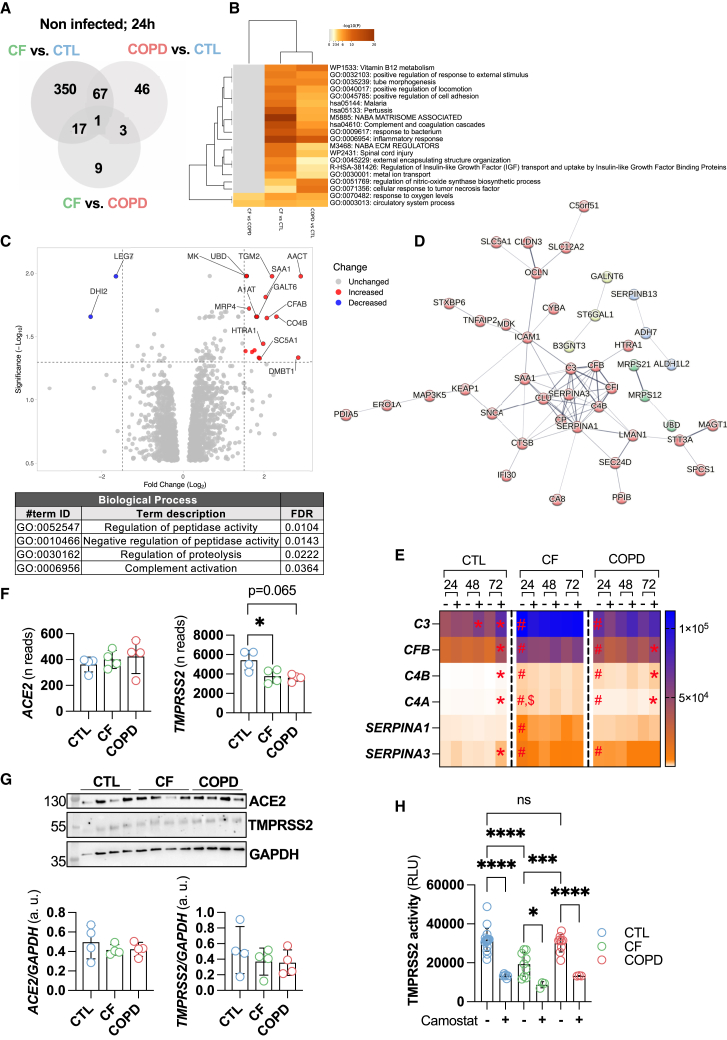
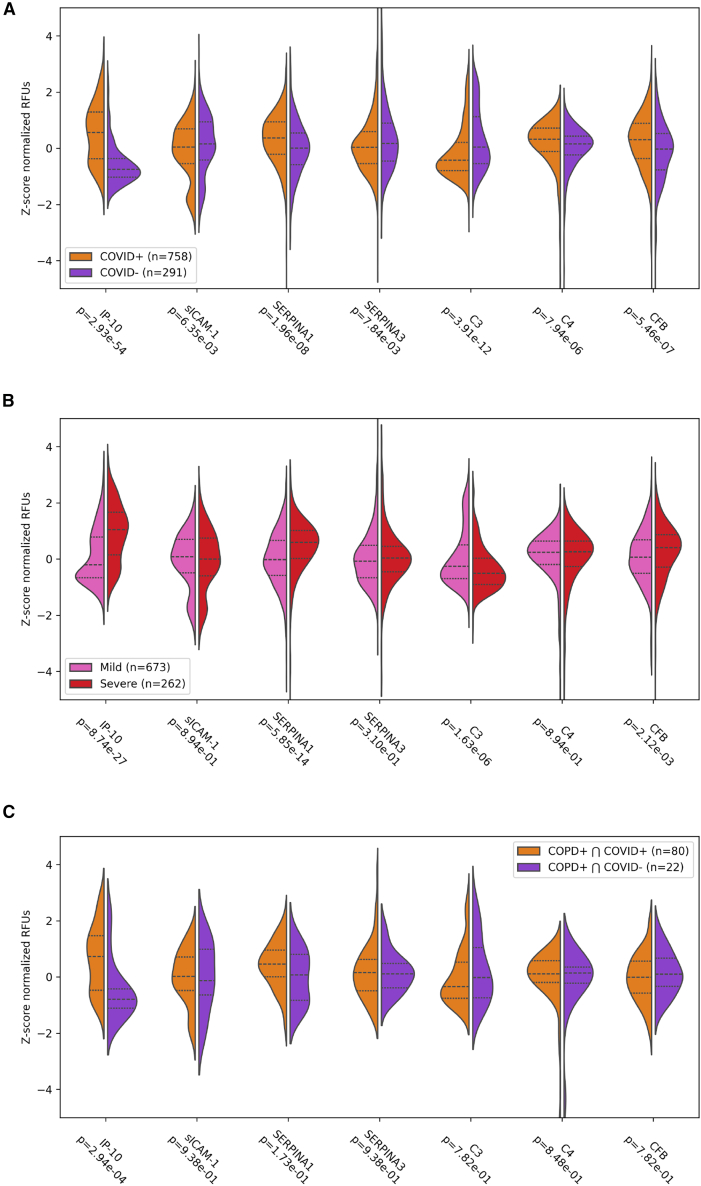
Pre-existing respiratory diseases may influence coronavirus disease (COVID-19) susceptibility and severity. However, the molecular mechanisms underlying the airway epithelial response to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection severity in patients with chronic respiratory diseases remain unelucidated. Using an in vitro model of differentiated primary bronchial epithelial cells, we aimed to investigate the molecular mechanisms of SARS-CoV-2 infection in pre-existing cystic fibrosis (CF) and chronic obstructive pulmonary disease (COPD). Our study revealed reduced susceptibility of CF and COPD airway epithelia to SARS-CoV-2, relative to that in healthy controls. Mechanistically, reduced transmembrane serine protease 2 (TMPRSS2) activity potentially contributed to this resistance of CF epithelium. Upregulated complement and inflammatory pathways in CF and COPD epithelia potentially primed the antiviral state prior to infection. Analysis of a COVID-19 patient cohort validated our findings, correlating specific inflammatory markers (IP-10, SERPINA1, and CFB) with COVID-19 severity. This study elucidates SARS-CoV-2 pathogenesis and identifies potential biomarkers for clinical monitoring.
Keywords: Microbiology; Respiratory medicine; Virology.
© 2025 The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Naehrlich L., Orenti A., Dunlevy F., Kasmi I., Harutyunyan S., Pfleger A., Keegan S., Daneau G., Petrova G., Tješić-Drinković D., et al. Incidence of SARS-CoV-2 in people with cystic fibrosis in Europe between February and June 2020. J. Cyst. Fibros. 2021;20:566–577. doi: 10.1016/j.jcf.2021.03.017. - DOI - PMC - PubMed
-
- Corvol H., de Miranda S., Dehillotte C., Lemonnier L., Chiron R., Danner-Boucher I., Hamidfar R., Houdouin V., Macey J., Marguet C., et al. Cumulative Incidence and Risk Factors for Severe Coronavirus Disease 2019 in French People With Cystic Fibrosis. Clin. Infect. Dis. 2022;75:2135–2144. doi: 10.1093/cid/ciac333. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
