

Comparative therapeutic efficacy and safety of first-line and second-line therapies for metastatic castration-resistant prostate cancer: a systematic review and network meta-analysis
- PMID: 40104085
- PMCID: PMC11914769
- DOI: 10.1016/j.eclinm.2025.103129
Comparative therapeutic efficacy and safety of first-line and second-line therapies for metastatic castration-resistant prostate cancer: a systematic review and network meta-analysis
Abstract
Background: There is no cross-sectional comparison on therapeutic and adverse effects for treatments of metastatic castration-resistant prostate cancer (mCRPCa). We aimed to horizontally compare them for all common first-line and second-line therapies.
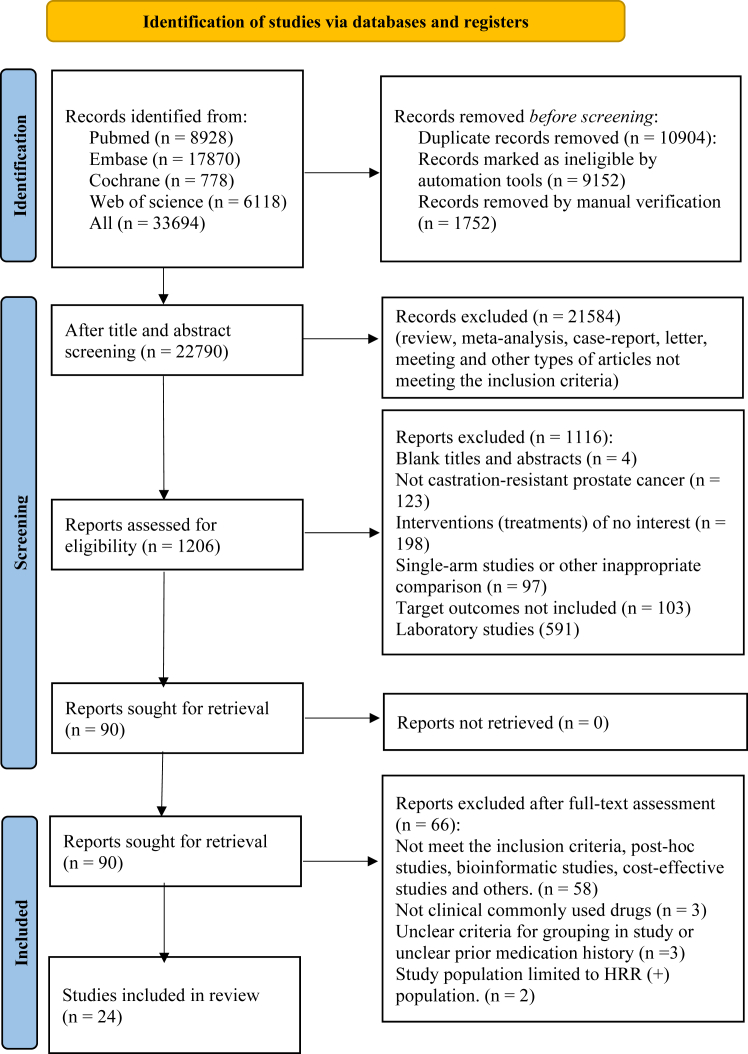
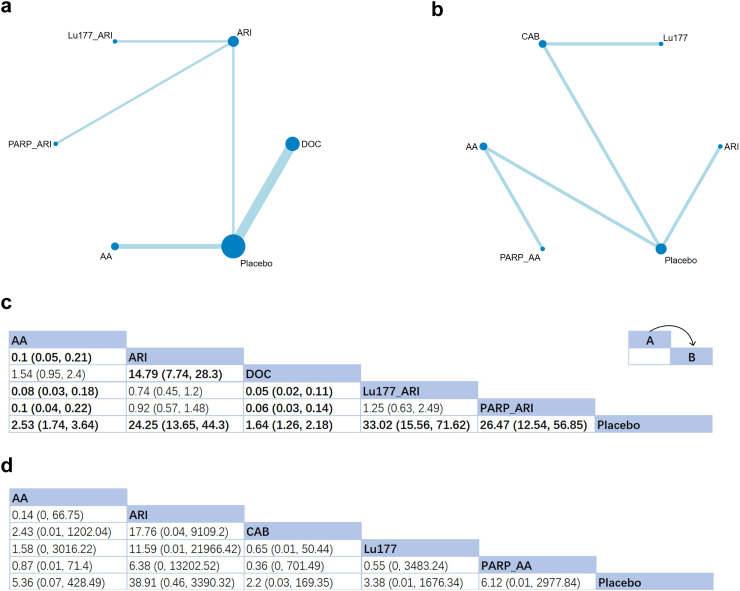
Methods: We conducted a network meta-analysis with a systematic review in four databases (Pubmed, Web of Science, Embase, and Cochrane Library) up to January 5th, 2025. All randomized controlled trials (RCT) related to mCRPCa treatments with a clear description in study design were included. Endpoints included the radiographic progression-free survival (rPFS), overall survival (OS), time to PSA progression (TTPP), PSA progression rate (PSARR), and adverse events. All data was extracted by two researchers and analyzed with Gemtc package in R and Stata15. This NMA protocol was registered online (ID: CRD42025633178).
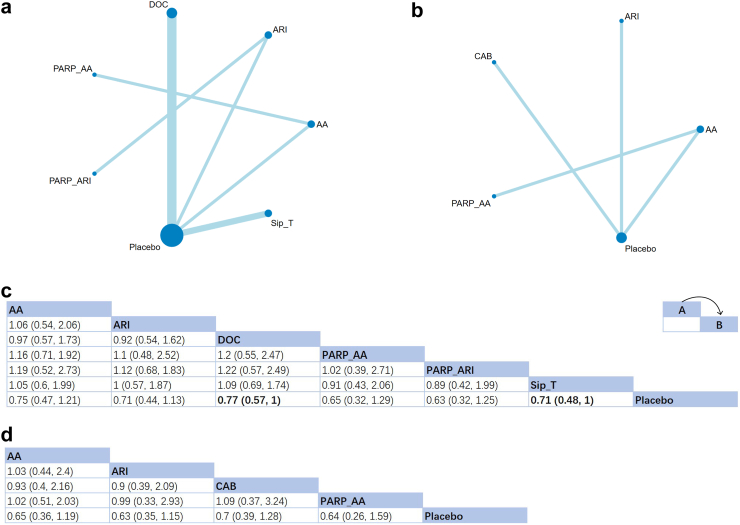
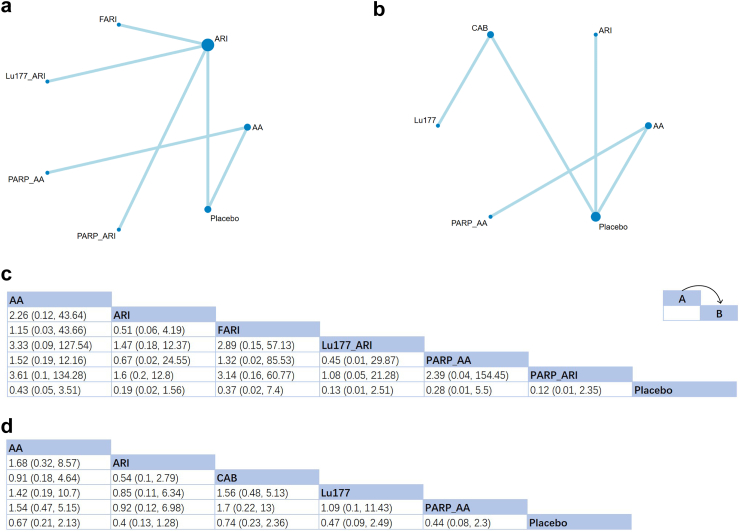
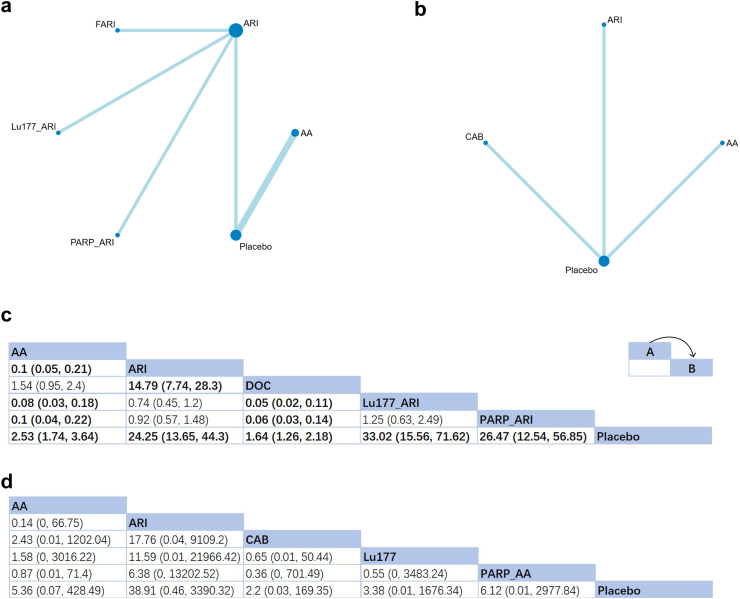
Findings: After screening among 33,694 articles, 24 RCTs involving 13,059 cases were included. For first-line treatments, combination therapies with second-generation androgen receptor inhibitors (ARIs) showed superior efficacies in OS [HR of poly(ADP-ribose) polymerase inhibitors (PARPi) + ARI: 0.63 (0.32,1.25)], TTPP [HR of Lu177 + ARI: 0.07 (0.01,0.87)] and PSARR [RR of Lu177 + ARI: 33.02 (15.56,71.62)] with the highest SUCRA (Surface under the Cumulative Ranking Curve) (72%, 91% and 97% respectively). PARPi + ARI also performed best for rPFS (SUCRA: 85%, with an insignificant HR [0.12 (0.02,2.35)]. For post-docetaxel second-line treatments, ARI also emerged as the preferred option. Efficacies of post-ARI second-line treatments were not evaluated due to the lack of related RCTs. No obvious heterogeneity and publication bias was detected during the therapeutic comparison.
Interpretation: This study provided comparative evidence for first-line and post-chemotherapy second-line mCRPCa treatment options. Second-generation ARIs exhibited good efficacy, particularly when combined with other treatments. However, the safety analysis necessitated balance between benefits and adverse events, especially for combination therapies. Stronger evidence is needed through direct comparisons in future clinical trials.
Funding: The study was supported by The National Natural Science Foundation of China (No. 82172568).
Keywords: First-line treatment; Metastatic castration-resistant prostate cancer; Network meta-analysis; Second-line treatment; Therapeutic effect.
© 2025 The Author(s).
Conflict of interest statement
We declare no competing interests.
Figures
References
-
- Bray F., Laversanne M., Sung H., et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. - PubMed
-
- Lowrance W., Dreicer R., Jarrard D.F., et al. Updates to advanced prostate cancer: AUA/SUO guideline (2023) J Urol. 2023;209(6):1082–1090. - PubMed
-
- Tilki D., van den Bergh R.C.N., Briers E., et al. EAU-EANM-ESTRO-ESUR-ISUP-SIOG guidelines on prostate cancer. Part II-2024 update: treatment of relapsing and metastatic prostate cancer. Eur Urol. 2024;86(2):164–182. - PubMed
-
- Schaeffer E.M., Srinivas S., Adra N., et al. NCCN Guidelines® insights: prostate cancer, version 3.2024. J Natl Compr Canc Netw. 2024;22(3):140–150. - PubMed
-
- Hutton B., Salanti G., Caldwell D.M., et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162(11):777–784. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
