

Assessment of heart and lung morphology in a single case during cardiopulmonary resuscitation: A virtual simulation
- PMID: 40104099
- PMCID: PMC11914767
- DOI: 10.1016/j.resplu.2025.100910
Assessment of heart and lung morphology in a single case during cardiopulmonary resuscitation: A virtual simulation
Abstract
Background: Basic science research in cardiopulmonary resuscitation (CPR) is limited by challenges in obtaining haemodynamic data from models that simulate physiological processes. In this study, we assessed the morphology of the heart and lungs and calculated the ejection fractions of cardiac chambers during CPR using a virtual simulation.
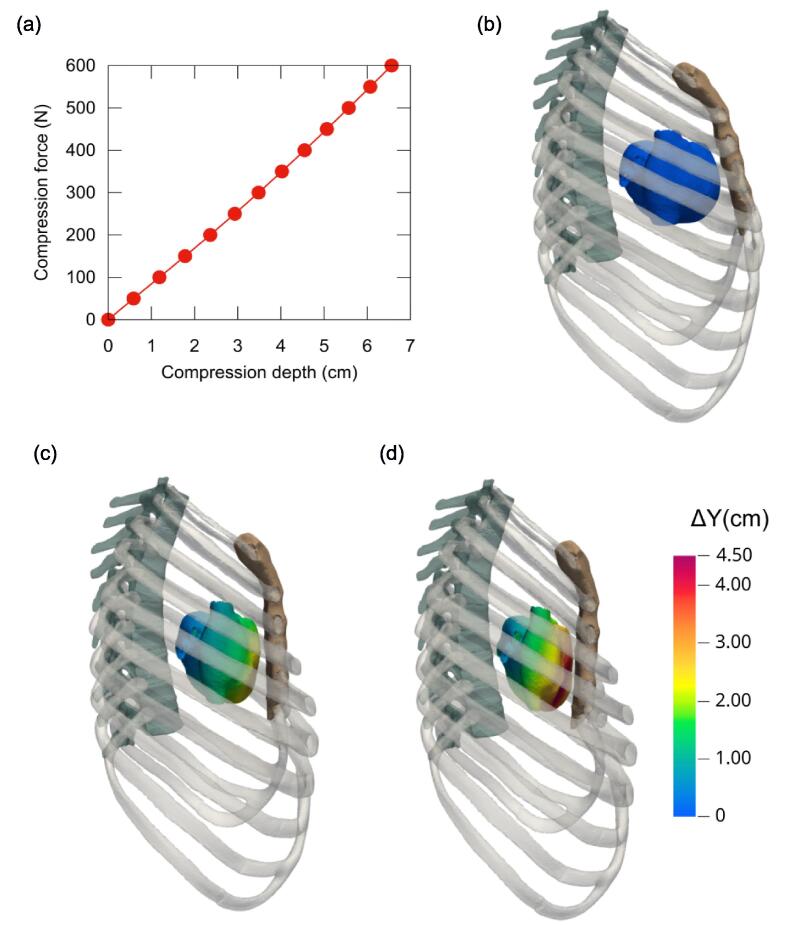
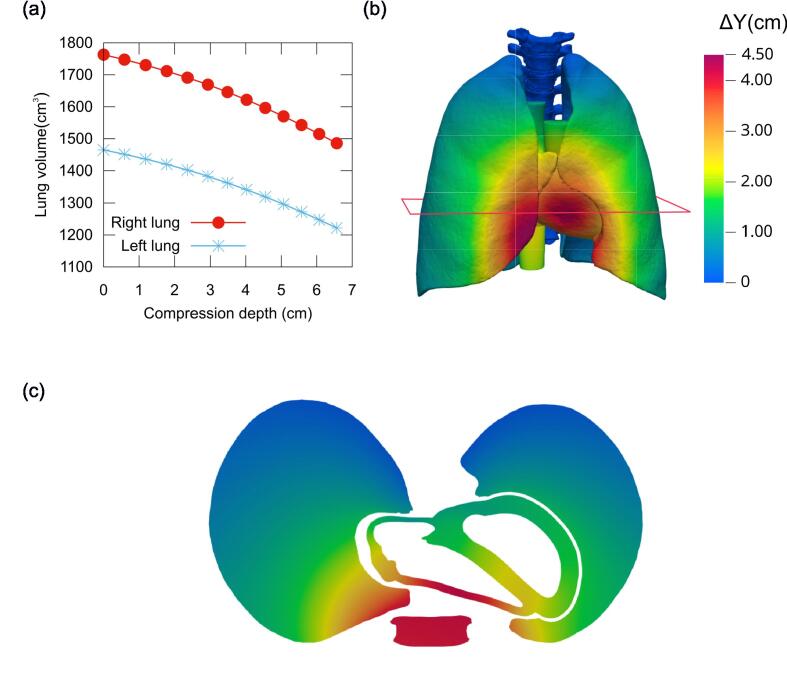
Methods: A finite element model of a complete thorax, including internal organs, thoracic rib cage, spine, musculature, and a generic material representing soft tissues, was constructed from magentic resonance images of a man. Twelve chest compression simulations were performed with forces ranging from F = 50 to 600 N. During compression, lung and heart volumes were assessed, and the ejection fraction of each cardiac chamber was calculated.
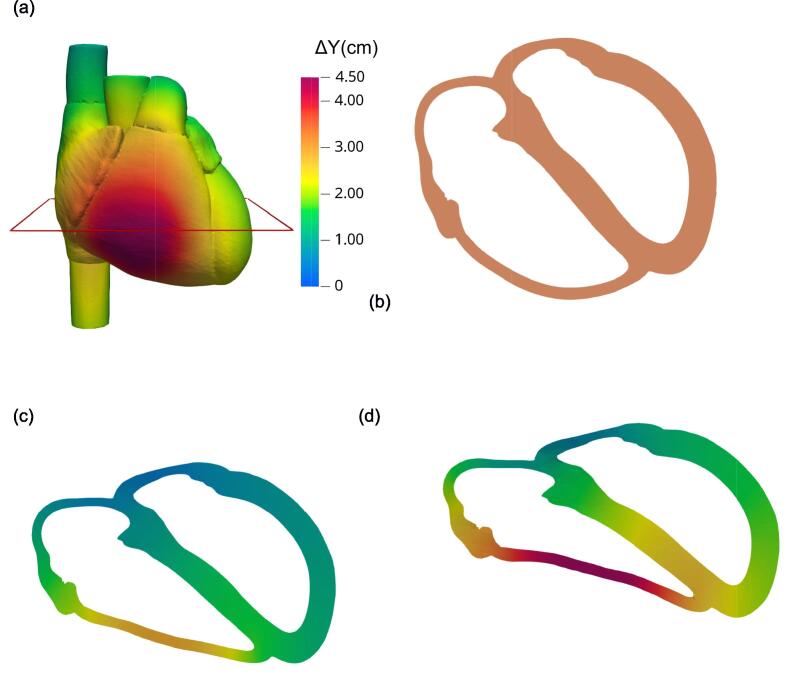
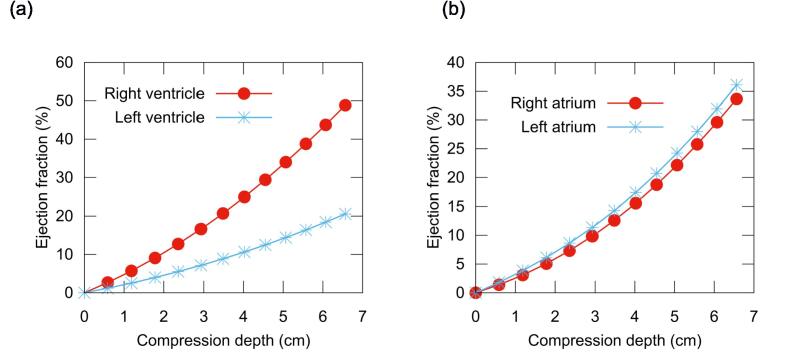
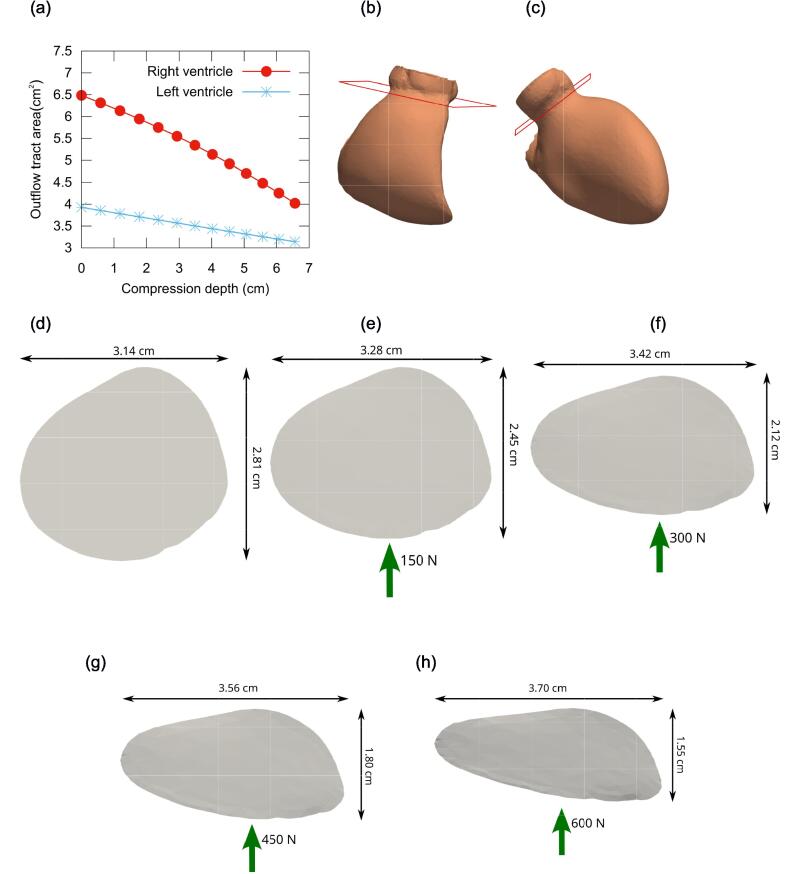
Results: In our numerical simulations a compression depth of 5.06 cm was reached with a force of 450 N. At this depth, the right and left ventricular ejection fractions were 34.0% and 14.4%, respectively, while the right and left atrial ejection fractions were 22.1% and 24.2%, respectively. The cross-sectional area of the outflow tract decreased by 27.5% and 15.6% in the right and left ventricles, respectively. Lung volumes decreased by 193 cm3 and 169 cm3 in the right and left lungs, respectively, representing 11.2% of the total lung volume.
Conclusion: The right ventricle exhibited the highest ejection fraction among the cardiac chambers, and the left atrium showed a higher ejection fraction than the left ventricle during CPR.
Keywords: Cardiopulmonary resuscitation; Finite element model; Haemodynamics.
© 2025 The Author(s).
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Association between left ventricular outflow tract opening and successful resuscitation after cardiac arrest.Resuscitation. 2019 May;138:8-14. doi: 10.1016/j.resuscitation.2019.02.027. Epub 2019 Feb 27. Resuscitation. 2019. PMID: 30825552
-
Relationship Between Left Ventricle Position and Haemodynamic Parameters During Cardiopulmonary Resuscitation in a Pig Model.Heart Lung Circ. 2018 Dec;27(12):1489-1497. doi: 10.1016/j.hlc.2017.08.020. Epub 2017 Sep 24. Heart Lung Circ. 2018. PMID: 29056259
-
The effect of thoracic dimensions on compression depth during cardiopulmonary resuscitation.Int J Numer Method Biomed Eng. 2023 Jul;39(7):e3718. doi: 10.1002/cnm.3718. Epub 2023 May 11. Int J Numer Method Biomed Eng. 2023. PMID: 37166223
-
Considerations for the Use of Intracardiac Echocardiography in Cardiac Arrest.Resuscitation. 2020 Apr;149:158-161. doi: 10.1016/j.resuscitation.2020.02.003. Epub 2020 Feb 25. Resuscitation. 2020. PMID: 32109504 Review.
-
2017 American Heart Association Focused Update on Pediatric Basic Life Support and Cardiopulmonary Resuscitation Quality: An Update to the American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care.Circulation. 2018 Jan 2;137(1):e1-e6. doi: 10.1161/CIR.0000000000000540. Epub 2017 Nov 6. Circulation. 2018. PMID: 29114009 Review.
References
-
- Tsao C.W., Aday A.W., Almarzooq Z.I., et al. Heart disease and stroke statistics—2022 update: a report from the American Heart Association. Circulation. 2022;145:e153–e639. - PubMed
-
- Gräsner J.T., Wnent J., Herlitz J., et al. Survival after out-of-hospital cardiac arrest in Europe – results of the EuReCa TWO study. Resuscitation. 2020;148:218–226. - PubMed
-
- Georgiou M., Papathanassoglou E., Xanthos T. Systematic review of the mechanisms driving effective blood flow during adult CPR. Resuscitation. 2014;85:1586–1593. - PubMed
-
- Sladen A. Landmark perspective: closed-chest massage, Kouwenhoven, Jude, Knickerbocker. JAMA. 1984;251:3137–3140. - PubMed
LinkOut - more resources
Full Text Sources
