

Maximal Intraoperative 5-Aminolevulinic Acid Fluorescence During Surgical Resection of Multiple Lesions in Multifocal Glioblastoma to Achieve Greater Extent of Resection: A Case Report
- PMID: 40104462
- PMCID: PMC11915777
- DOI: 10.7759/cureus.79083
Maximal Intraoperative 5-Aminolevulinic Acid Fluorescence During Surgical Resection of Multiple Lesions in Multifocal Glioblastoma to Achieve Greater Extent of Resection: A Case Report
Abstract
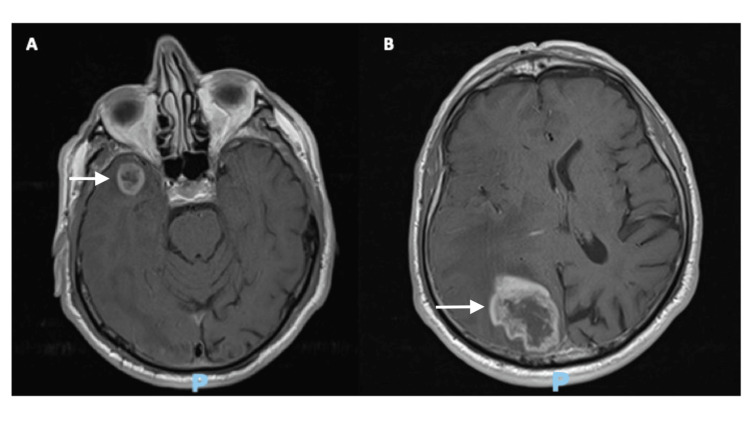
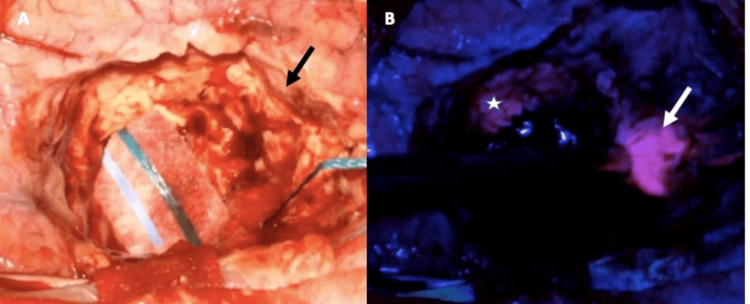
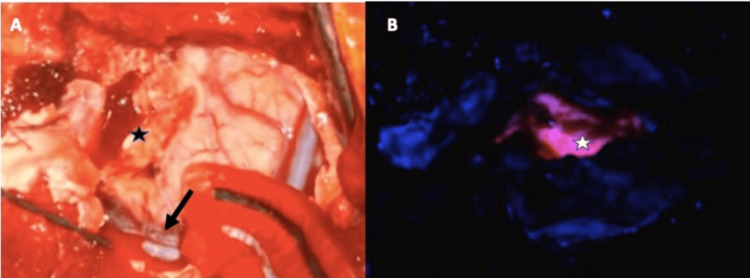
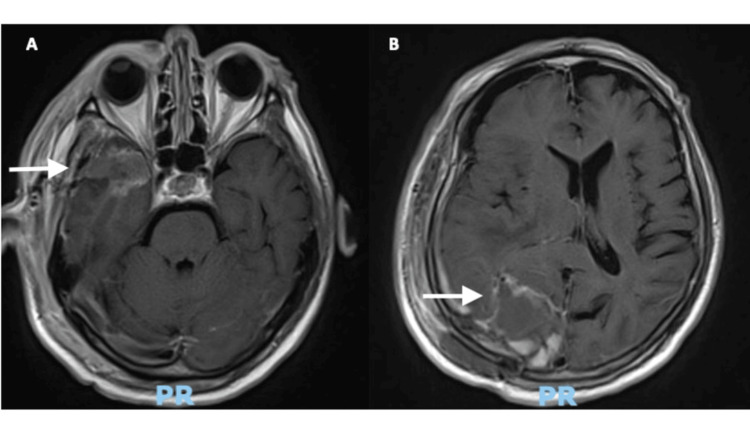
Multifocal glioblastoma represents a therapeutic challenge with conflicting evidence on treatment, though it appears that the extent of resection also plays an important role in this disease. The use of 5-aminolevulinic acid has been shown to improve the extent of resection in high-grade gliomas; however, there is little information about its use in multifocal glioblastoma. We present the case of a 79-year-old patient with distant glial lesions who underwent surgery for the resection of a right temporal and a right occipital lesion at the same surgical time. Intraoperative findings and postsurgical events are described in this report. This case shows that resection of multiple lesions in a patient with multifocal glioblastoma using intraoperative 5-aminolevulinic acid fluorescence is feasible and safe.
Keywords: 5-ala; fluorescence; glioblastoma; multifocal; surgery.
Copyright © 2025, Jacobo et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
A prospective Phase II clinical trial of 5-aminolevulinic acid to assess the correlation of intraoperative fluorescence intensity and degree of histologic cellularity during resection of high-grade gliomas.J Neurosurg. 2016 May;124(5):1300-9. doi: 10.3171/2015.5.JNS1577. Epub 2015 Nov 6. J Neurosurg. 2016. PMID: 26544781 Clinical Trial.
-
Impact of the combination of 5-aminolevulinic acid-induced fluorescence with intraoperative magnetic resonance imaging-guided surgery for glioma.World Neurosurg. 2011 Jul-Aug;76(1-2):120-7. doi: 10.1016/j.wneu.2011.02.005. World Neurosurg. 2011. PMID: 21839963
-
5-aminolevulinic enhanced brain lesions mimic glioblastoma: A case report and literature review.Medicine (Baltimore). 2024 Jan 5;103(1):e34518. doi: 10.1097/MD.0000000000034518. Medicine (Baltimore). 2024. PMID: 38181251 Free PMC article. Review.
-
5-Aminolevulinic Acid Hydrochloride (5-ALA)-Guided Surgical Resection of High-Grade Gliomas: A Health Technology Assessment.Ont Health Technol Assess Ser. 2020 Mar 6;20(9):1-92. eCollection 2020. Ont Health Technol Assess Ser. 2020. PMID: 32194883 Free PMC article.
-
Clinical utility of 5-aminolevulinic acid HCl to better visualize and more completely remove gliomas.Onco Targets Ther. 2016 Sep 12;9:5629-42. doi: 10.2147/OTT.S97030. eCollection 2016. Onco Targets Ther. 2016. PMID: 27672334 Free PMC article. Review.
References
-
- The oncological role of resection in newly diagnosed diffuse adult-type glioma defined by the WHO 2021 classification: a review by the RANO resect group. Karschnia P, Gerritsen JK, Teske N, ey al. Lancet Oncol. 2024;25:404. - PubMed
-
- Supramaximal resection: retrospective study on IDH-wildtype glioblastomas based on the new RANO-resect classification. Tropeano MP, Raspagliesi L, Bono BC, et al. Acta Neurochir (Wien) 2024;166:196. - PubMed
-
- Use of 5-ALA fluorescence-guided surgery versus white-light conventional microsurgery for the resection of newly diagnosed glioblastomas (RESECT study): a French multicenter randomized phase III study. Picart T, Pallud J, Berthiller J, et al. J Neurosurg. 2024;140:987–1000. - PubMed
Publication types
LinkOut - more resources
Full Text Sources